

Implications of a new clinical classification of acute myocardial infarction
- PMID: 39824208
- PMCID: PMC11929527
- DOI: 10.1093/ehjacc/zuaf002
Implications of a new clinical classification of acute myocardial infarction
Abstract
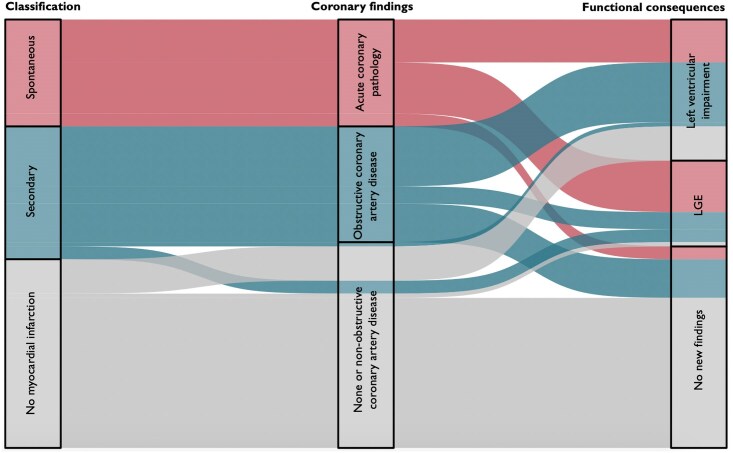
Aims: The diagnostic criteria for Type 2 myocardial infarction identify a heterogeneous group of patients with variable outcomes and no clear treatment implications. We aimed to determine the implications of a new clinical classification for myocardial infarction with more objective diagnostic criteria using cardiac imaging.
Methods and results: In a prospective cohort study, patients with Type 2 myocardial infarction underwent coronary angiography and cardiac magnetic resonance imaging or echocardiography. The new classification was applied to identify (i) spontaneous myocardial infarction due to acute coronary pathology, (ii) secondary myocardial infarction precipitated by acute illness in the presence of obstructive coronary artery disease, a new regional wall motion abnormality, or infarct-pattern scarring, and (iii) no myocardial infarction in the absence of obstructive disease or new myocardial abnormality. In 100 patients (65 years, 43% women) with Type 2 myocardial infarction, the new classification identified 25 and 31 patients with spontaneous and secondary myocardial infarction, respectively, and 44 without myocardial infarction. Compared with patients without myocardial infarction, those with secondary myocardial infarction were older, had more risk factors, and had higher troponin concentrations (P < 0.05 for all). During a median follow-up of 4.4 years, death, myocardial infarction, or heart failure hospitalization was more common in secondary myocardial infarction compared with those without myocardial infarction [55% (17/31) vs. 16% (7/44), P < 0.001].
Conclusion: A new clinical classification of myocardial infarction informed by cardiac imaging would reduce the diagnosis of myocardial infarction in acute illness and identify those patients at highest risk who are most likely to benefit from treatment.
Clinical trial registration: https://clinicaltrials.gov/ct2/show/NCT03338504.
Keywords: Cardiac troponin; Coronary artery disease; Imaging; Myocardial infarction.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: J.B. has received honoraria from Siemens, Roche Diagnostics, Ortho Clinical Diagnostics, Quidel Corporation, and Beckman Coulter, and travel support from Medtronic, all outside the submitted work. M.C.W. has received speaker fees from Cannon Medical Systems, Siemens Healthineers, and Novartis. N.L.M. reports receiving honoraria from Abbott Diagnostics, Siemens Healthineers, and Roche Diagnostics. All other authors have no interests to declare.
Figures


Comment in
-
Implications of a new clinical classification of acute myocardial infarction.Eur Heart J Acute Cardiovasc Care. 2025 Aug 7;14(8):504-506. doi: 10.1093/ehjacc/zuaf065. Eur Heart J Acute Cardiovasc Care. 2025. PMID: 40305765 Free PMC article. No abstract available.
References
-
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth universal definition of myocardial infarction (2018). Circulation 2018;138:e618–e651. - PubMed
-
- Sandoval Y, Jaffe AS. Type 2 myocardial infarction: JACC review topic of the week. J Am Coll Cardiol 2019;73:1846–1860. - PubMed
-
- McCarthy CP, Januzzi JL Jr, Gaggin HK. Type 2 myocardial infarction: an evolving entity. Circ J 2018;82:309–315. - PubMed
-
- Bularga A, Taggart C, Mendusic F, Kimenai DM, Wereski R, Lowry MTH, et al. Assessment of oxygen supply-demand imbalance and outcomes among patients with type 2 myocardial infarction: a secondary analysis of the high-STEACS cluster randomized clinical trial. JAMA Netw Open 2022;5:E2220162. - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- FS/16/75/32533/BHF_/British Heart Foundation/United Kingdom
- MRC_/Medical Research Council/United Kingdom
- Swiss Academy of Medical Sciences
- Gottfried and Julia Bangerter-Rhyner Foundation
- WT103782AIA/WT_/Wellcome Trust/United Kingdom
- Edinburgh Doctoral College Scholarship
- University Hospital of Basel
- Division of Internal Medicine
- University of Basel
- 15/JTA/Sir Jules Thorn Award for Biomedical Science
- MR/V007254/1/Clinical Research Training
- FS/CRTF/21/2473/Clinical Research Training Fellowship
- SNSF_/Swiss National Science Foundation/Switzerland
- WT_/Wellcome Trust/United Kingdom
- CH/09/002/26360/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
