

Evaluating the effectiveness of handheld ultrasound in primary blast lung injury: a comprehensive study
- PMID: 39824921
- PMCID: PMC11742448
- DOI: 10.1038/s41598-025-86928-6
Evaluating the effectiveness of handheld ultrasound in primary blast lung injury: a comprehensive study
Abstract
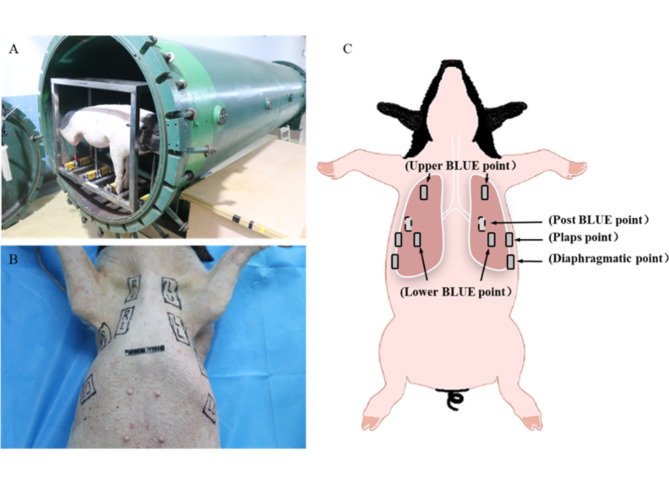
The incidence of blast injuries has been rising globally, particularly affecting the lungs due to their vulnerability. Primary blast lung injury (PBLI) is associated with high morbidity and mortality rates, while early diagnostic methods are limited. With advancements in medical technology, and portable handheld ultrasound devices, the efficacy of ultrasound in detecting occult lung injuries early remains unclear. This study evaluates the effectiveness of immediate lung ultrasound in diagnosing PBLI. The study involved 25 healthy male Bama mini-pigs subjected to BST-I-type biological shock wave tubes. The pigs were randomly assigned to non-injured and injured groups with driving pressures of 4.0 MPa, 4.5 MPa, and 4.8 MPa. Four PBLI models were created: no injury, minor, moderate, serious and severe. Immediate lung ultrasound following the BLUE-PLUS protocol and arterial blood gas analysis were conducted pre-injury and 0.5 h, 3 h, 6 h, 12 h, and 24 h post-injury, respectively. The study analyzed lung ultrasound score differences and their correlations with lung function parameters, using ROC analysis to determine early diagnostic standards and mortality prediction efficacy. The study found that in cases of moderate and severe PBLI, lung ultrasound scores and AaDO2 significantly increased at 0.5 h post-injury, while PaO2 decreased. There was good consistency between left and right lung ultrasound results at all times. Lung ultrasound scores were significantly correlated with PaO2 and AaDO2 but not with PaCO2. The scores accurately predicted injury severity at various time points within 24 h post-injury, and the 0.5 h lung ultrasound score predicted 24 h mortality with 95.8% efficiency. PBLI exhibits hidden severity, necessitating improved early diagnostics. Immediate lung ultrasound provides effective differentiation for moderate and severe PBLI at multiple time points within 24 h post-injury, is easy to implement, and offers effective mortality risk prediction as early as 0.5 h post-injury. These findings underscore lung ultrasound's significant clinical application value in pre-hospital early treatment settings for PBLI.
Keywords: BLUE-PLUS protocol; Lung function; Point-of-care ultrasound (POCUS); Primary blast lung injury; Shock wave tube; Ultrasound.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical approval and consent to participate: All experimental procedures were conducted in strict accordance with the Guide for the Care and Use of Laboratory Animals established by the Animal Ethics Committee of the Army Medical University (AMUWEC20223478) and complied with Directive 2010/63/EU of the European Parliament. The animal production license number is SCXK (Chongqing) 2017-0002, and the animal use license number is SYXK (Chongqing) 2017-0002. The care and handling of the animals were conducted in strict accordance with the guidelines outlined in the “Guide for the Care and Use of Laboratory Animals“( https://www.nature.com/srep/journal-policies/editorial-policies#experimental-subjects ). All surgeries were performed with ketamine hydrochloride, propofol and sufentanil citrate anesthesia, and all efforts were made to minimize suffering. All methods were performed in accordance with the relevant guidelines and regulations. The study was carried out in compliance with the ARRIVE guidelines ( https://arriveguidelines.org ).
Figures







Similar articles
-
Dynamic pathophysiological features of early primary blast lung injury: a novel functional incapacity pig model.Eur J Trauma Emerg Surg. 2025 Jan 24;51(1):60. doi: 10.1007/s00068-024-02672-y. Eur J Trauma Emerg Surg. 2025. PMID: 39856331 Free PMC article.
-
Value of lung ultrasound score for evaluation of blast lung injury in goats.Chin J Traumatol. 2020 Feb;23(1):38-44. doi: 10.1016/j.cjtee.2019.11.005. Epub 2020 Jan 11. Chin J Traumatol. 2020. PMID: 32005413 Free PMC article.
-
[Changes of arterial blood gas indexes of free-field primary blast lung injury of pigs and its application value].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021 Dec;33(12):1466-1470. doi: 10.3760/cma.j.cn121430-20210809-01154. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021. PMID: 35131014 Chinese.
-
Crosstalk between Inflammation and Hemorrhage/Coagulation Disorders in Primary Blast Lung Injury.Biomolecules. 2023 Feb 10;13(2):351. doi: 10.3390/biom13020351. Biomolecules. 2023. PMID: 36830720 Free PMC article. Review.
-
Damage-Associated Molecular Patterns and Their Signaling Pathways in Primary Blast Lung Injury: New Research Progress and Future Directions.Int J Mol Sci. 2020 Aug 31;21(17):6303. doi: 10.3390/ijms21176303. Int J Mol Sci. 2020. PMID: 32878118 Free PMC article. Review.
References
-
- Depalma, R. G. et al. Blast injuries. N. Engl. J. Med.352(13), 1335–1342 (2005). - PubMed
-
- Wolf, S. J. et al. Blast injuries. Lancet (London, England)374(9687), 405–415 (2009). - PubMed
-
- Scott, T. E. et al. Primary Blast Lung Injury: The UK Military Experience. Mil. Med.185(5–6), e568–e572 (2020). - PubMed
-
- Scott, T. E. et al. Primary blast lung injury—a review. Br. J. Anaesth.118(3), 311–316 (2017). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
