

Diffuseness of coronary artery disease impacts on immediate hemodynamic and predicted clinical outcomes
- PMID: 39825017
- PMCID: PMC11742033
- DOI: 10.1038/s41598-025-85872-9
Diffuseness of coronary artery disease impacts on immediate hemodynamic and predicted clinical outcomes
Abstract
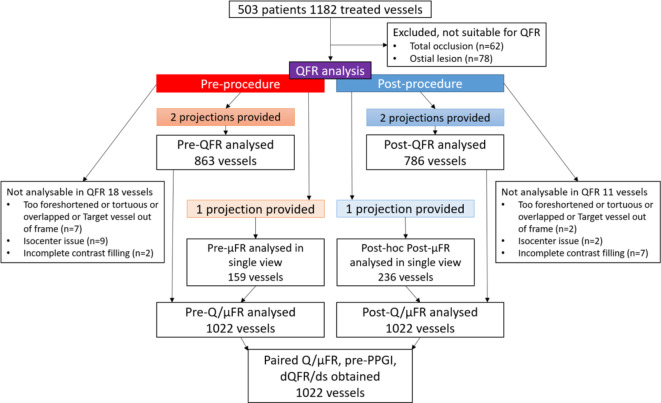
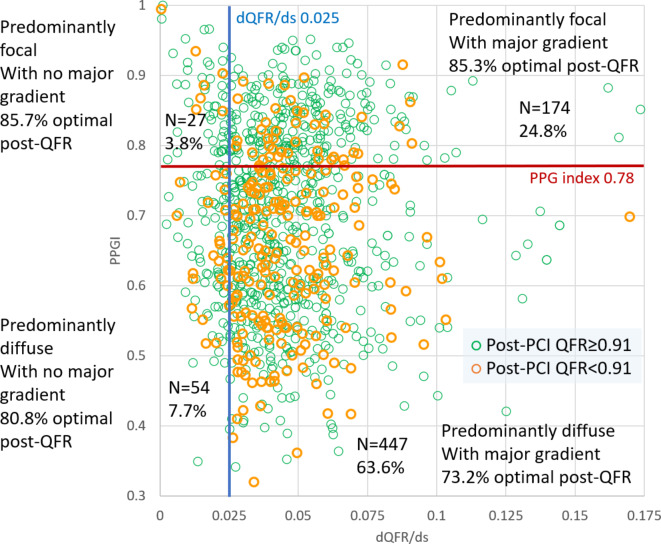
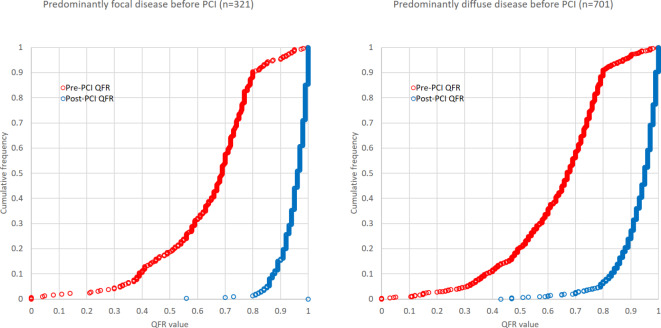
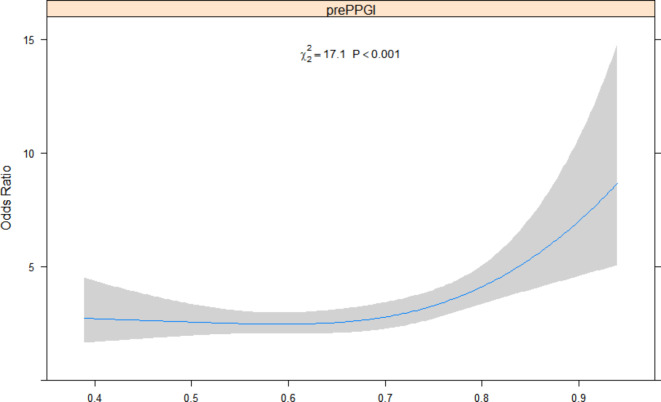
Diffuse coronary artery disease (CAD) impacts the immediate hemodynamic and clinical outcomes of percutaneous coronary intervention (PCI). We evaluated whether the diffuse pattern of CAD derived from angiographic Quantitative flow ratio (QFR) impacts the immediate hemodynamic outcome post-PCI and the medium term predicted vessel-oriented composite endpoint (VOCE). Paired pre-procedure QFRs were assessed in 503 patients and 1022 vessels in the Multivessel TALENT (MVT) trial. The pathophysiological pattern of CAD was defined as "predominantly diffuse" or "focal" according to a virtual QFR pullback pressure gradient (PPG) index < 0.78 and ≥ 0.78, respectively. Physiological "focal severity" was assessed using the QFR gradient per mm (dQFR/ds), with a value ≥ 0.025/mm the threshold for a "major gradient". A post-PCI QFR ≥ 0.91 was considered optimal. Median pre-PCI PPG index was 0.70 (IQR 0.59-0.80). The prevalence of "predominantly diffuse" CAD and "major gradient" were 68.6% and 85.8%, respectively. A "Predominantly diffuse" pattern with a major gradient had a higher risk of a post-PCI QFR < 0.91 (OR 1.52,95%CI 1.47-1.58). In multivariable analysis, low QFR PPG index (diffuse disease) was an independent determinant of a post-PCI QFR < 0.91 (per 0.1 decrease of QFR PPG index, OR:9.8, 95% CI 3.0-32.2, p < 0.001). Based on post-PCI QFR the predicted 2-year VOCE, a powered endpoint in the MVT trial, was 6.1% and 4.2% in diffuse and focal lesions, respectively. A pre-procedure physiological pattern of diffuse CAD is an independent determinant of an unfavourable immediate hemodynamic outcome post-PCI, and detrimentally affects the predicted 2-year VOCE.Clinical Trial Registration URL: https://www.clinicaltrials.gov/ct2/show/NCT04390672 Unique Identifier: NCT04390672 (registration date 15/05/2020).
Keywords: Acute coronary syndrome; Chronic coronary syndrome; Coronary artery disease; Disease pattern; Drug-eluting stent; Multiple vessel disease; Percutaneous coronary intervention; Quantitative flow ratio.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: Dr Serruys reports institutional grants from Philips/Volcano, SMT, Novartis, Xeltis, Merillife, outside the submitted work. Dr Tu reports research grants and consultancy from Pulse Medical. Dr Sabaté has received consultant fees from Abbott Vascular and Ivascular outside the submitted work. Dr Möllmann reports speaker honoraria from Abbott, Boston Scientific, and SMT. All other authors have no conflict of interest to declare.
Figures
References
-
- Serruys, P. W., Kageyama, S., Garg, S. & Onuma, Y. In the beginning there was angina pectoris, at the end there was still angina pectoris. JACC Cardiovasc. Interv.15, 2519–2522 (2022). - PubMed
-
- Kogame, N. et al. The impact of coronary physiology on contemporary clinical decision making. Jacc-Cardiovasc. Interv.13, 1617–1638 (2020). - PubMed
-
- Biscaglia, S. et al. Invasive coronary physiology after stent implantation. Jacc-Cardiovasc. Interven.14, 237–246 (2021). - PubMed
-
- Tebaldi, M. et al. Evolving routine standards in invasive hemodynamic assessment of coronary stenosis The Nationwide Italian SICI-GISE cross-sectional ERIS study. Jacc-Cardiovasc. Interven.11, 1482–1491 (2018). - PubMed
-
- Kogame, N. et al. Clinical implication of quantitative flow ratio after percutaneous coronary intervention for 3-vessel disease. Jacc-Cardiovasc. Interven.12, 2064–2075 (2019). - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
