

Immunotherapy-Resistant Neuropathic Pain and Fatigue Predict Quality-of-Life in Contactin-Associated Protein-Like 2 Antibody Disease
- PMID: 39825737
- PMCID: PMC11831874
- DOI: 10.1002/ana.27177
Immunotherapy-Resistant Neuropathic Pain and Fatigue Predict Quality-of-Life in Contactin-Associated Protein-Like 2 Antibody Disease
Abstract
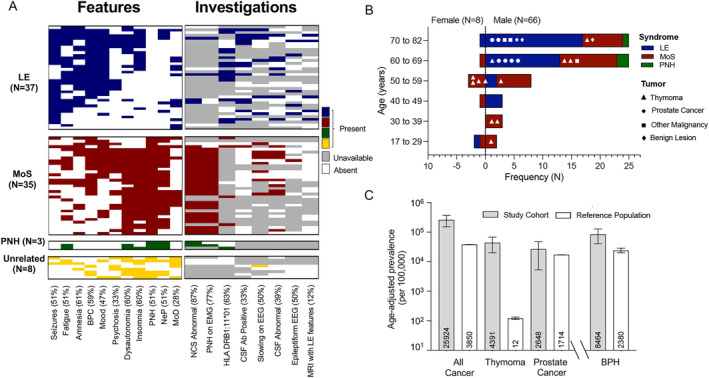
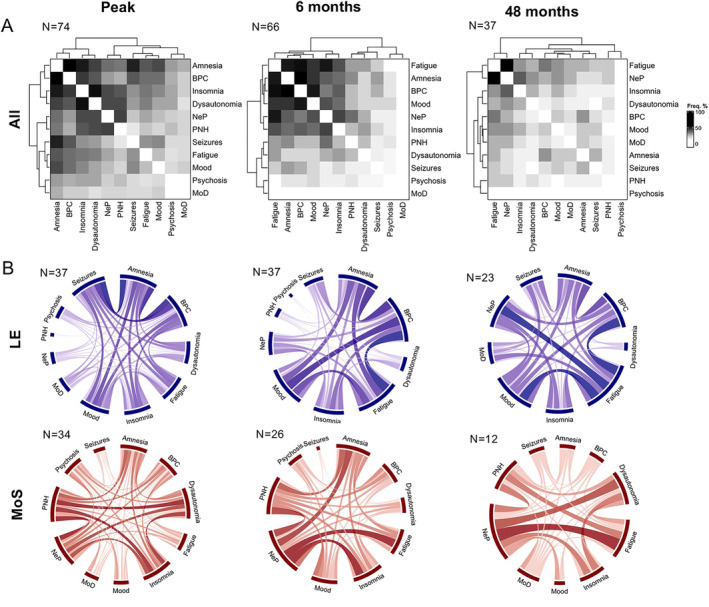
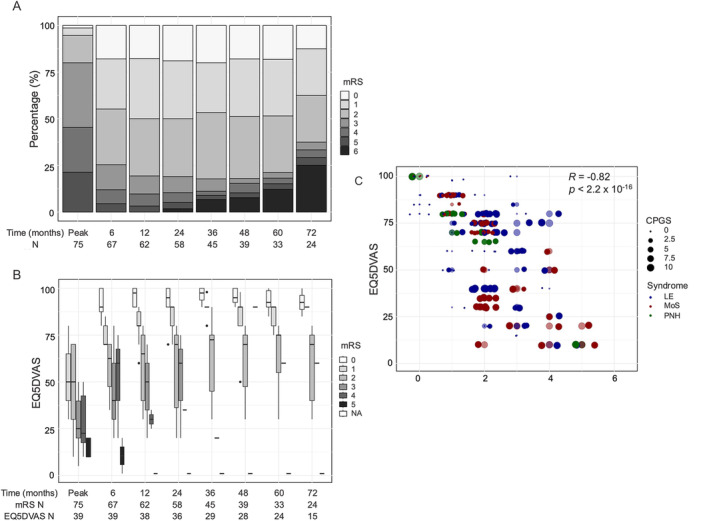
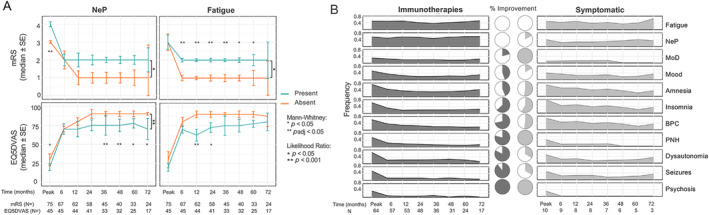
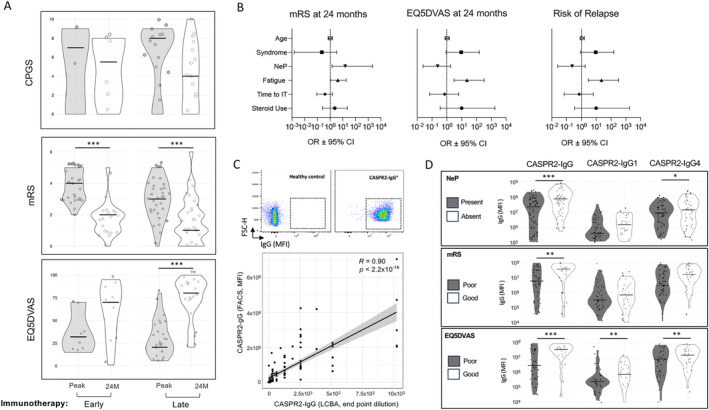
The long-term clinical outcomes and associated prognostic factors in contactin-associated protein-like 2 (CASPR2)-antibody diseases are unknown. A total of 75 participants with CASPR2 antibodies were longitudinally assessed for disability, quality-of-life, and chronic pain. Although most symptoms improved within 6 months of treatment, neuropathic pain and fatigue were the most immunotherapy refractory, and persisted for up to 6 years. Furthermore, these two factors-but not CASPR2 antibody levels or subclasses-independently predicted worse disability and quality-of-life at 24 months. Quality-of-life varied widely for any given modified Rankin Scale score, indicating a divergence between patient and clinician assessed outcomes. Further work should study the relative importance of these measures, and the immunopathogenesis underlying intractable symptoms. ANN NEUROL 2025;97:521-528.
© 2025 The Author(s). Annals of Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
S.B. is named on a patent application entitled “Diagnostic Strategy to improve specificity of CASPR2 antibody detection” (TBA / BB Ref. JA94536P.GBA)”. D.L.B. has a patent application “A method for the treatment or prevention of pain, or excessive neuronal activity, or epilepsy”, Application No. 16/337,428. S.R.I. receives licensed royalties on patent application WO/2010/046716 entitled “Neurological Autoimmune Disorders,” and has filed two other patents entitled “Diagnostic method and therapy” (WO2019211633 and US app 17/051,930; PCT application WO202189788A1) and “Biomarkers” (WO202189788A1, US App 18/279,624; PCT/GB2022/050614).
Figures
Similar articles
-
Association of Leucine-Rich Glioma Inactivated Protein 1, Contactin-Associated Protein 2, and Contactin 2 Antibodies With Clinical Features and Patient-Reported Pain in Acquired Neuromyotonia.JAMA Neurol. 2018 Dec 1;75(12):1519-1527. doi: 10.1001/jamaneurol.2018.2681. JAMA Neurol. 2018. PMID: 30242309 Free PMC article.
-
Anti-contactin-associated protein-2 encephalitis: relevance of antibody titres, presentation and outcome.Eur J Neurol. 2017 Jan;24(1):175-186. doi: 10.1111/ene.13180. Epub 2016 Oct 27. Eur J Neurol. 2017. PMID: 27786401
-
Leucine-Rich Glioma-Inactivated 1 versus Contactin-Associated Protein-like 2 Antibody Neuropathic Pain: Clinical and Biological Comparisons.Ann Neurol. 2021 Oct;90(4):683-690. doi: 10.1002/ana.26189. Epub 2021 Aug 30. Ann Neurol. 2021. PMID: 34370313 Free PMC article.
-
Anti-contactin-associated protein-like 2 antibody-associated cerebellar ataxia: A case report and literature review.J Neuroimmunol. 2021 Apr 15;353:577515. doi: 10.1016/j.jneuroim.2021.577515. Epub 2021 Feb 3. J Neuroimmunol. 2021. PMID: 33640718 Review.
-
Systematic review of the clinical spectrum of CASPR2 antibody syndrome.J Neurol. 2020 Apr;267(4):1137-1146. doi: 10.1007/s00415-019-09686-2. Epub 2020 Jan 7. J Neurol. 2020. PMID: 31912210
References
-
- Irani SR, Alexander S, Waters P, et al. Antibodies to Kv1 potassium channel‐complex proteins leucine‐rich, glioma inactivated 1 protein and contactin‐associated protein‐2 in limbic encephalitis, Morvan's syndrome and acquired neuromyotonia. Brain 2010;133:2734–2748. 10.1093/brain/awq213. - DOI - PMC - PubMed
-
- Muñiz‐Castrillo S, Joubert B, Elsensohn M‐H, et al. Anti‐CASPR2 clinical phenotypes correlate with HLA and immunological features. J Neurol Neurosurg Psychiatry 2020;91:1076–1084. https://jnnp.bmj.com/content/91/10/1076. - PubMed
MeSH terms
Substances
Grants and funding
- Association of British Neurologists
- University of Oxford
- National Institute for Health Research
- Advanced Pain Discovery Platform
- 104079/Z/14/Z/WT_/Wellcome Trust/United Kingdom
- 102176/Z/13/Z/WT_/Wellcome Trust/United Kingdom
- British Medical Association, Margaret Temple Vera Down
- The Petre Foundation
- WT_/Wellcome Trust/United Kingdom
- Faculty of Medicine, University of British Columbia
- Guarantors of Brain
- MR/X022013/1/MRC_/Medical Research Council/United Kingdom
- P1201/Epilepsy Research UK
- BRAIN Foundation
- European Union Horizon 2020
- NIHR Oxford Biomedical Research Centre
- MR/V007173/1/MRC_/Medical Research Council/United Kingdom
- National Health and Medical Research Council
- AMS_/Academy of Medical Sciences/United Kingdom
- University of Sydney
- Royal Australasian College of Physicians
- Fulbright US-UK Commission, MS Society research award
LinkOut - more resources
Full Text Sources
Medical
