

SD-OCT-histopathologic correlation in Schnabel's cavernous optic nerve atrophy
- PMID: 39827237
- PMCID: PMC11978856
- DOI: 10.1038/s41433-025-03603-w
SD-OCT-histopathologic correlation in Schnabel's cavernous optic nerve atrophy
Abstract
Background: Until now, Schnabel's cavernous optic nerve atrophy (SCONA) has solely been a histopathological diagnosis exhibiting variable degrees of optic nerve (ON) atrophy with characteristic cavernous spaces filled with acid mucopolysaccharides. We report the first correlation of histopathologic findings with spectral domain-optical coherence tomography (SD-OCT) imaging in SCONA.
Methods: We examined the eye of an index patient with histopathologically identified SCONA who had undergone multimodal imaging before enucleation for iris ring melanoma. The extent of SCONA in the index patient and three other enucleated eyes with SCONA were determined histopathologically. The histopathological findings of our index patient were correlated with in vivo SD-OCT images before enucleation and compared to representative images from eyes with a normal versus glaucomatous optic disc.
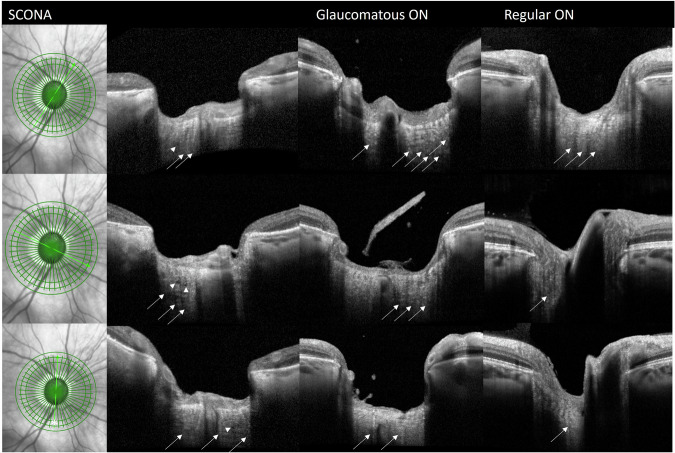
Results: Histopathologic examination of our index patient showed a pre- and intralaminar extension of SCONA. Atrophy of the inner retinal layers was observed corresponding to the extent of SCONA. Correlation with SD-OCT showed small intralaminar hyporeflective pseudocysts which were detected in multiple scans corresponding to the histologically affected areas. These changes were neither visible in scans of patients with glaucomatous atrophy nor those with a normal ON.
Conclusions: We present the first correlation of clinical and pathological findings in SCONA and were able to identify distinct SD-OCT characteristics for this condition. These findings may help to detect SCONA in vivo and to study this rare entity clinically with regard to its clinical course, risk factors, and pathogenesis. However, more cases of SCONA are needed to confirm our findings.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: FGH, TA: Consultant for Heidelberg Engineering. MCH-C (non-financial): Secretary of the International Society of Ophthalmic Pathology (ISOP), Member of the section committee “Ophthalmic Pathology” within the German Ophthalmological Society (DOG), Member of the “Annual Meeting Program Committee” of ARVO for the section “Anatomy Pathology (AP)”. Ethics: This study involves human participants and was approved by an Ethics Committee. All our patients sign an informed consent that the histologic sections can be used for study purposes. This was approved by the Ethics Committee of the University of Bonn (328/16).
Figures



Similar articles
-
Appearance of Schnabel's Cavernous Degeneration of the Optic Nerve: Four Weeks Before Enucleation for Melanoma.Ophthalmology. 2015 Dec;122(12):2531. doi: 10.1016/j.ophtha.2015.10.021. Ophthalmology. 2015. PMID: 26592675 No abstract available.
-
[Comparison of scanning laser polarimetry, optical coherence tomography 1 and Stratus optical coherence tomography for the detection of axonal loss in band atrophy of the optic nerve].Arq Bras Oftalmol. 2006 Jul-Aug;69(4):531-7. doi: 10.1590/s0004-27492006000400014. Arq Bras Oftalmol. 2006. PMID: 17119726 Portuguese.
-
Optic disc morphometry with optical coherence tomography: comparison with planimetry of fundus photographs and influence of parapapillary atrophy and pigmentary conus.Indian J Ophthalmol. 2005 Sep;53(3):187-91. doi: 10.4103/0301-4738.16678. Indian J Ophthalmol. 2005. PMID: 16137964
-
[New insights into the study of optic nerve diseases].Nippon Ganka Gakkai Zasshi. 2013 Mar;117(3):187-210; discussion 211. Nippon Ganka Gakkai Zasshi. 2013. PMID: 23631254 Review. Japanese.
-
Optical Coherence Tomography Neuro-Toolbox for the Diagnosis and Management of Papilledema, Optic Disc Edema, and Pseudopapilledema.J Neuroophthalmol. 2021 Mar 1;41(1):77-92. doi: 10.1097/WNO.0000000000001078. J Neuroophthalmol. 2021. PMID: 32909979 Free PMC article. Review.
References
-
- Schnabel I. Das glaukomatöse Sehnervenleiden. Arch Augenheilkd. 1892;24:273–92.
-
- Schnabel I. Die glaukomatöse Sehnervenatrophie. Wien Med Wochenschr. 1900:1170.
-
- Schnabel I. Die Entwicklungsgeschichte der glaucomatösen Exkavation. Opthalmologica. 1905;14:1–22.
-
- Giarelli L, Falconieri G, Cameron JD, Pheley AM. Schnabel cavernous degeneration: a vascular change of the aging eye. Arch Pathol Lab Med. 2003;127:1314–9. - PubMed
-
- Gong H, Ye W, Freddo TF, Hernandez MR. Hyaluronic acid in the normal and glaucomatous optic nerve. Exp Eye Res. 1997;64:587–95. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
