

Superior biomechanical stability of pedicle screws compared to lateral mass screws: recommendations for bicortical positioning and enhancing bone contact in geriatric C1 vertebrae
- PMID: 39827360
- PMCID: PMC11742196
- DOI: 10.1186/s13018-025-05472-1
Superior biomechanical stability of pedicle screws compared to lateral mass screws: recommendations for bicortical positioning and enhancing bone contact in geriatric C1 vertebrae
Abstract
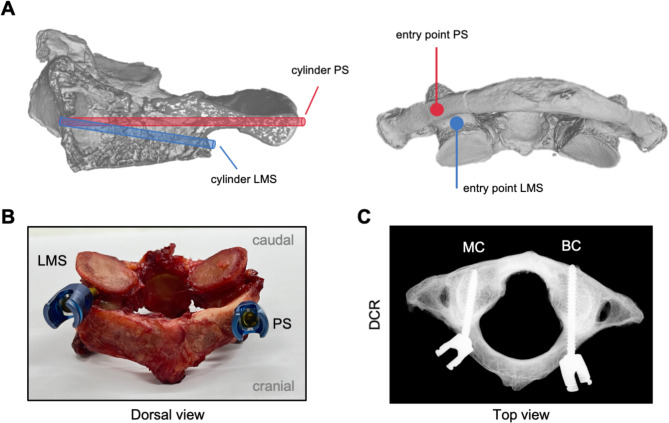
Background: In atlantoaxial instabilities, posterior C1/C2 fusion using lateral mass screws (LMS) or pedicle screws (PS) in a mono- or bicortical position in the atlas is a typical treatment. The bone microstructure and positioning of the screw trajectories appear to be of significant relevance for stability.
Purpose: The aim of this study was a comparative analysis of the mechanical durability of screw fixation concerning microstructural characteristics of the trajectories of LMS and PS in mono- and bicortical position.
Methods: Human C1 from geriatric body donors (n = 28; 50% female, age 80.8 ± 13.9 years) were collected and characterized based on their bone microstructure. Additionally, the mechanical stability of LMS and PS fixation in mono- and bicortical positioning was tested by mechanical loading. High-resolution quantitative computed tomography was used to analyze the bone microstructure of cylinders corresponding to the trajectories of PS and LMS in mono- and bicortical locations in each C1. After instrumentation with both screw types and types of fixation, the mechanical stability was tested by increased cyclic loading in cranio-caudal direction.
Results: Trajectories of PS presented with more bone volume and a higher contact length to cortical bone. Simultaneously, a higher number of cycles and a higher maximum force was needed to loosen PS compared to LMS, while the loose by torque at the experiment end was still greater in PS. Differences between mono- and bicortical positioning of PS and LMS have only been observed in the initial stiffness of screws. When comparing microstructural and mechanical properties, the cortical contact length and bone volume in screw trajectories were strongest associated with a high loose and cycle count.
Conclusions: This study suggests that mono- and bicortical positioning of PS is similarly efficient in creating a stable basis for screw fixation in the atlas. While PS are superior to LMS, the contact with cortical bone is of major relevance for a stable foundation.
Keywords: Bone microstructure; C1; Cervical spine surgery; Lateral mass screw; Mechanical testing; Pedicle screw.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was reported to the local ethics committee (2022-300148-WF) and complied with the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures




Similar articles
-
C1 pedicle screws versus C1 lateral mass screws: comparisons of pullout strengths and biomechanical stabilities.Spine (Phila Pa 1976). 2009 Feb 15;34(4):371-7. doi: 10.1097/BRS.0b013e318193a21b. Spine (Phila Pa 1976). 2009. PMID: 19214096
-
Biomechanical Effects of Lateral Inclination C1 and C2 Pedicle Screws on Atlantoaxial Fixation.Orthop Surg. 2021 Oct;13(7):2027-2033. doi: 10.1111/os.13137. Epub 2021 Sep 20. Orthop Surg. 2021. PMID: 34541829 Free PMC article.
-
Comparison of fatigue strength of C2 pedicle screws, C2 pars screws, and a hybrid construct in C1-C2 fixation.Spine (Phila Pa 1976). 2014 Jan 1;39(1):E12-9. doi: 10.1097/BRS.0000000000000063. Spine (Phila Pa 1976). 2014. PMID: 24108297
-
Anatomic considerations for the pedicle screw placement in the first cervical vertebra.Spine (Phila Pa 1976). 2005 Jul 1;30(13):1519-23. doi: 10.1097/01.brs.0000168546.17788.49. Spine (Phila Pa 1976). 2005. PMID: 15990666 Clinical Trial.
-
Impact of Starting Point and Bicortical Purchase of C1 Lateral Mass Screws on Atlantoaxial Fusion: Meta-Analysis and Review of the Literature.J Spinal Disord Tech. 2015 Aug;28(7):242-53. doi: 10.1097/BSD.0b013e31828ffc97. J Spinal Disord Tech. 2015. PMID: 23563339 Review.
References
-
- Lomoschitz FM, Blackmore CC, Mirza SK, Mann FA. Cervical spine injuries in patients 65 years old and older: epidemiologic analysis regarding the effects of age and injury mechanism on distribution, type, and stability of injuries. AJR Am J Roentgenol. 2002;178:573–7. - PubMed
-
- Tarawneh A, Taqvi S, Salem K, Sahota O. Cervical spine fragility fractures in older people: 5-year experience at a regional spine centre. Age Ageing. 2020;49:1102–4. - PubMed
-
- Ryan MD, Henderson JJ. The epidemiology of fractures and fracture-dislocations of the cervical spine. Injury. 1992;23:38–40. - PubMed
-
- Dailey AT, Hart D, Finn MA, Schmidt MH, Apfelbaum RI. Anterior fixation of odontoid fractures in an elderly population. J Neurosurg Spine. 2010;12:1–8. - PubMed
-
- Pearson AM, Martin BI, Lindsey M, Mirza SK. C2 vertebral fractures in the Medicare Population: incidence, outcomes, and costs. J Bone Joint Surg Am. 2016;98:449–56. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
