

RADAR - Radiomics on aSDH: predicting outcome with surface area
- PMID: 39828870
- PMCID: PMC11743400
- DOI: 10.1007/s00701-024-06408-0
RADAR - Radiomics on aSDH: predicting outcome with surface area
Abstract
Background: Acute subdural hematoma is a critical condition, leading to significant morbidity and mortality. Despite advancements in surgical techniques, a portion of patients only show limited clinical improvement post-evacuation. Surgical intervention decisions are critically important, as they can either improve or worsen a patient's condition. Radiomics offers significant potential by extracting complex patterns from digital medical images and transforming them into high-dimensional data that reflect the underlying pathophysiology. By integrating Radiomics with individual patient characteristics, we can develop decision support models. This study aims to analyze radiomic parameters of aSDH to determine whether they support the decision to proceed with urgent surgery or opt for a conservative approach. We hypothesized that surface area could be a significant predictor of neurological outcome such as maintaining independent mobility (mRS ≥ 3) and survival rates.
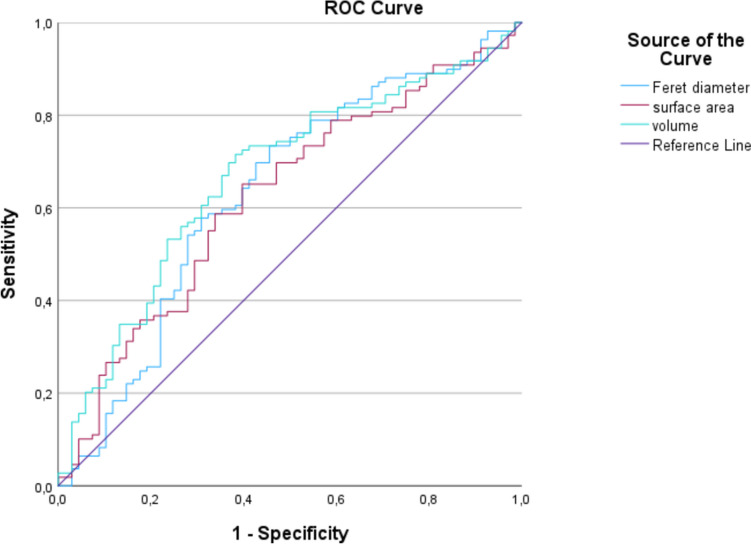
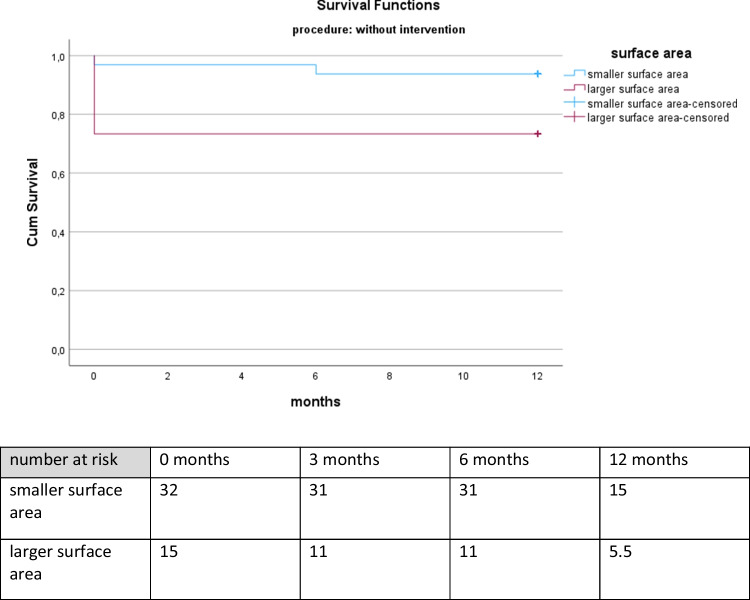
Methods: This retrospective study involved radiomic analysis according to neurological outcome and survival. Radiomic parameters were measured using 3D Slicer software. Statistical analyses explored correlations, employing AUC-analysis and Kaplan-Meier survival.
Results: Our findings revealed significant correlations between hematoma and surface area with poorer neurological prognosis. Further subgroup analysis showed surface area as a significant predictor for poorer outcomes in patients undergoing craniotomy (p = 0.006 in univariant- and p = 0.020 in multivariant analysis). In the total cohort, among conservatively managed and craniotomy subgroups, survival analysis highlighted an advantageous survival for patients exhibiting smaller surface areas (< 339.50 cm2).
Conclusions: Especially in craniotomy patients, surface area emerged as a possible predictor for neurological outcome and survival.
Keywords: Acute subdural hematoma; Outcome; Radiomics; Surface area.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical standards: All procedures performed in studies involving human participants were in accordance with the ethical standards of the Clinical Ethics Committee of the University of Leipzig (approval number 362/23-ek) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors. Due to the retrospective character of this study, formal consent is not required. We confirm the use of the relevant reporting checklist for this study. The study was not registered. Competing interests: The authors declare no competing interests.
Figures



Similar articles
-
PROMISE: Prognostic Radiomic Outcome Measurement in Acute Subdural Hematoma Evacuation Post-Craniotomy.Brain Sci. 2025 Jan 10;15(1):58. doi: 10.3390/brainsci15010058. Brain Sci. 2025. PMID: 39851426 Free PMC article.
-
KEPPRA: Key Epilepsy Prognostic Parameters with Radiomics in Acute Subdural Hematoma Before Craniotomy.Brain Sci. 2025 Feb 16;15(2):204. doi: 10.3390/brainsci15020204. Brain Sci. 2025. PMID: 40002536 Free PMC article.
-
Based on hematoma and perihematomal tissue NCCT imaging radiomics predicts early clinical outcome of conservatively treated spontaneous cerebral hemorrhage.Sci Rep. 2024 Aug 9;14(1):18546. doi: 10.1038/s41598-024-69249-y. Sci Rep. 2024. PMID: 39122887 Free PMC article.
-
Effectiveness of Craniectomy Versus Craniotomy in the Management of Acute Subdural Hematoma Patients: A Systematic Review.Cureus. 2024 Dec 16;16(12):e75842. doi: 10.7759/cureus.75842. eCollection 2024 Dec. Cureus. 2024. PMID: 39691407 Free PMC article. Review.
-
Decompressive craniectomy versus craniotomy for acute subdural hematoma: Updated meta-analysis of real-world clinical outcome after RESCUE-ASDH trial.J Trauma Acute Care Surg. 2024 Aug 1;97(2):299-304. doi: 10.1097/TA.0000000000004243. Epub 2024 Jan 10. J Trauma Acute Care Surg. 2024. PMID: 38197651
References
-
- Ahmed E, Aurangzeb A, Khan SA et al (2012) Frequency of conservatively managed traumatic acute subdural haematoma changing into chronic subdural haematoma. J Ayub Med Coll Abbottabad 24(1):71–74 - PubMed
-
- Akbik OS, Starling RV, Gahramanov S, Zhu Y, Lewis J (2019) Mortality and functional outcome in surgically evacuated acute subdural hematoma in elderly patients. World Neurosurg 126:e1235–e1241. 10.1016/j.wneu.2019.02.234 - PubMed
-
- Alessandri B, Nishioka T, Heimann A, Bullock RM, Kempski O (2006) Caspase-dependent cell death involved in brain damage after acute subdural hematoma in rats. Brain Res 1111(1):196–202. 10.1016/j.brainres.2006.06.105 - PubMed
-
- Aromatario M, Torsello A, D’Errico S et al (2021) Traumatic epidural and subdural hematoma: epidemiology, outcome, and dating. Med (Kaunas) 57(2):125. 10.3390/medicina57020125. https://www.mdpi.com/1648-9144/57/2/125 - PMC - PubMed
-
- Baechli H, Behzad M, Schreckenberger M, Buchholz HG, Heimann A, Kempski O, Alessandri B (2010) Blood constituents trigger brain swelling, tissue death, and reduction of glucose metabolism early after acute subdural hematoma in rats. J Cereb Blood Flow Metab 30(3):576–585. 10.1038/jcbfm.2009.230. Epub 2009 Nov 4. PMID: 19888286; PMCID: PMC2949142 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
