

Effectiveness of Cognitive Rehabilitation in Improving Symptoms and Restoring Cognitive Functions in Patients with Depression: An Updated Meta-Analysis of Randomized Controlled Trials
- PMID: 39830048
- PMCID: PMC11736863
- DOI: 10.5152/alphapsychiatry.2024.241731
Effectiveness of Cognitive Rehabilitation in Improving Symptoms and Restoring Cognitive Functions in Patients with Depression: An Updated Meta-Analysis of Randomized Controlled Trials
Abstract
Objective: Patients with depression often experience cognitive impairments. Cognitive rehabilitation, as an adjunctive intervention, may help to improve symptoms and restore functions in these patients. This study explores the effectiveness of cognitive rehabilitation in improving symptoms and restoring cognitive functions in patients with depression.
Methods: The following databases were systematically searched for relevant randomized controlled trials (RCTs): PubMed, Embase, and the Cochrane Central Register of Controlled Trials. Two reviewers independently screened the studies. The search was conducted from the inception of the databases to April 10, 2024. Standardized mean differences (SMDs) with 95% CIs, confidence interval were calculated using RevMan v. 5.3 software, and heterogeneity was assessed using Cochran's Q test and the I 2 statistic.
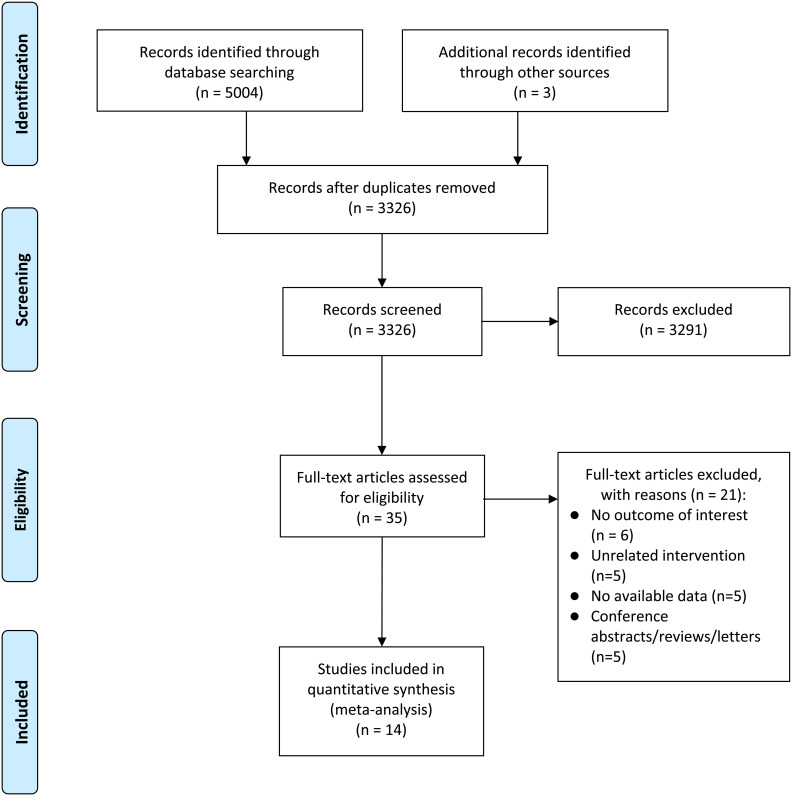
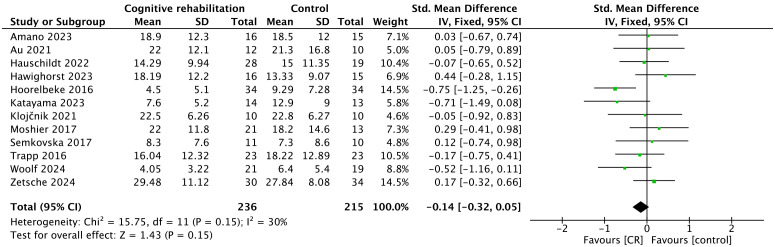
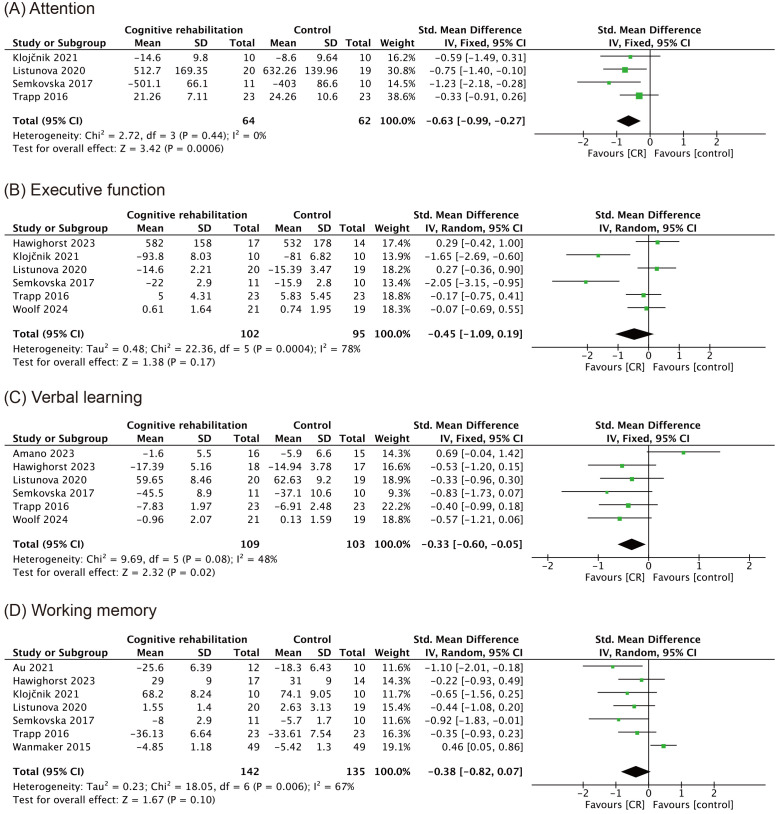
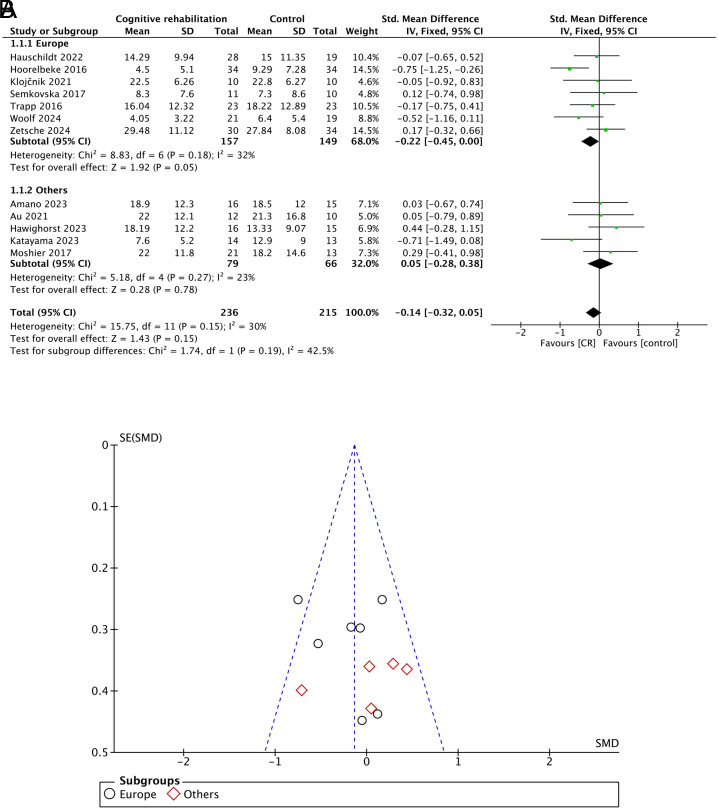
Results: A total of 14 RCTs involving 700 patients were included in this meta-analysis. Compared with the control group, there was no significant difference in the severity of depression after cognitive rehabilitation intervention, with a pooled SMD of -0.14 (95% CI: -0.32 to 0.05; P = .15; I2 = 30%). Among the 4 studies reporting attention-related data, cognitive rehabilitation significantly improved attention function in patients with depression compared with the control group, with an SMD of -0.63 (95% CI: -0.99 to -0.27; P < .001; I2 = 0%). In 6 studies, data showed significant improvement in verbal learning ability in patients with depression after cognitive rehabilitation intervention, with an SMD of -0.33 (95% CI: -0.60 to -0.05; P = .02; I2 = 48%). Executive function outcomes were reported in 6 studies, whereas working memory outcomes were reported in 7 studies, both before and after the intervention. No significant differences were observed between the groups, with SMDs of -0.45 (95% CI: -1.09 to 0.19; P = .17; I2 = 78%) in executive function and -0.38 (95% CI: -0.82 to 0.07; P = .10; I2 = 67%) in working memory post-intervention. Subgroup analysis suggested that cognitive rehabilitation training had a close to statistically significant improvement effect on depression severity in European regions, whereas no significant impact was observed in other regions.
Conclusion: Cognitive rehabilitation shows certain value in improving attention and verbal learning in patients with depression as an adjunctive treatment, but its effectiveness in improving depressive symptoms, executive function, and working memory remains inconclusive. Future large-sample RCTs are needed to further explore this aspect.
Keywords: Depression; cognitive function; executive function; meta-analysis.
2024 authors.
Conflict of interest statement
Declaration of Interests: The authors have no conflict of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous