

Spontaneous echo contrast in the left atrial appendage is linked to a higher risk of thromboembolic events and mortality in patients with atrial fibrillation
- PMID: 39830732
- PMCID: PMC11742588
- DOI: 10.1016/j.ijcha.2024.101590
Spontaneous echo contrast in the left atrial appendage is linked to a higher risk of thromboembolic events and mortality in patients with atrial fibrillation
Abstract
Background: Cardioversion, a rhythm control treatment for atrial fibrillation (AF), requires ruling out cardiac embolic sources, often originating from the left atrial appendage (LAA). Transesophageal echocardiography (TEE) is used for LAA evaluation, but it is invasive and not widely available. This study aimed to identify cardiovascular risk factors linked to LAA abnormalities and predictors of thromboembolic events and all-cause mortality.
Methods: A single-center retrospective analysis included AF patients admitted to the University Hospital Würzburg between 2009 and 2018 undergoing TEE.
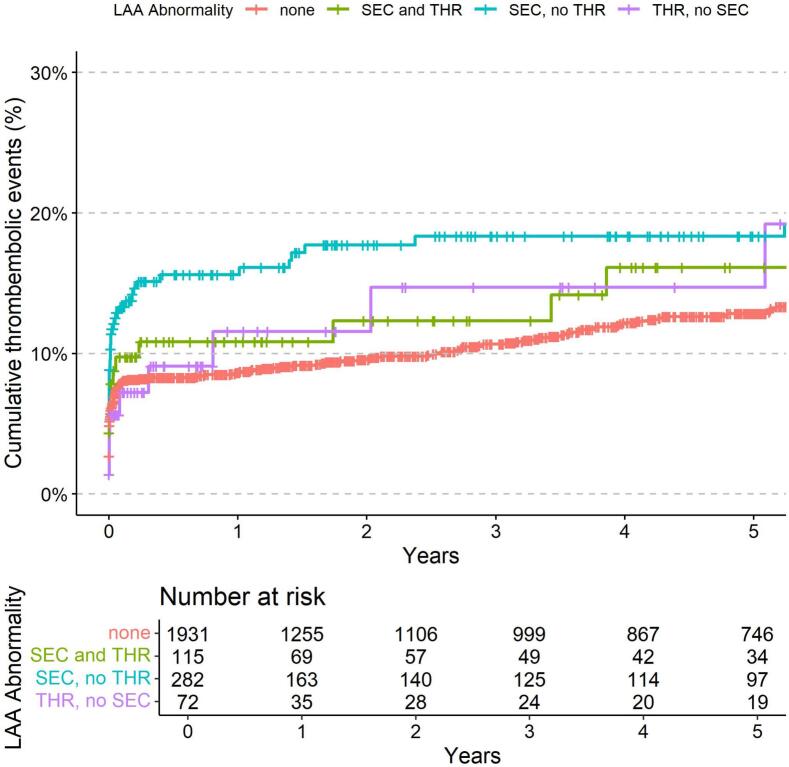
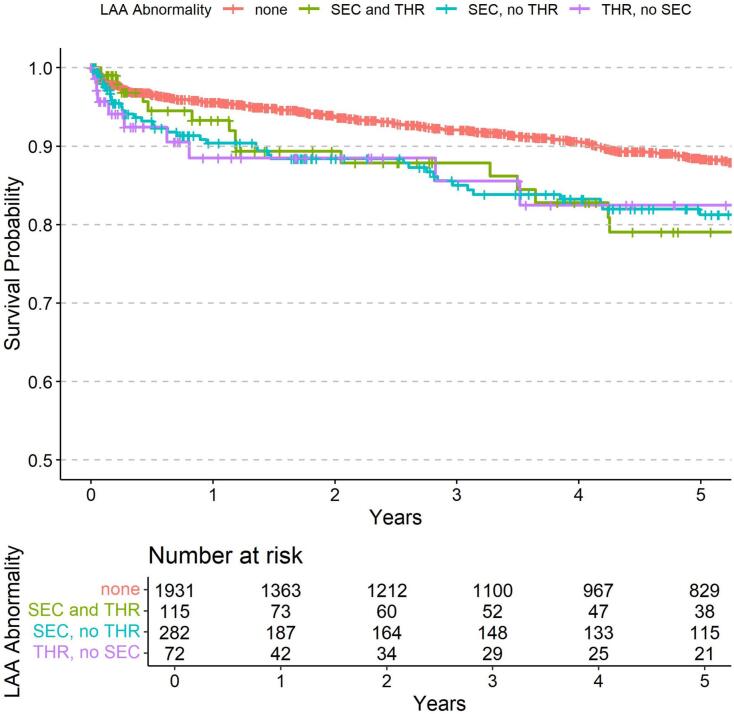
Results: Among 2400 AF patients (median age 72; 36 % women), 469 (20 %) had LAA abnormalities: 282 (60 %) had spontaneous echo contrast (SEC), 72 (15 %) had thrombus formation (THR), and 115 (25 %) had both. Predictors of LAA abnormalities included age (OR 1.04; p = 0.002), congestive heart failure (OR 1.70; p = 0.009), diabetes (OR 1.74; p = 0.007), stroke history (OR 3.36; p = 0.001), vascular disease (OR 1.57; p = 0.026), elevated alkaline phosphatase (OR 1.15; p = 0.003), prior VKA intake (OR 1.53; p = 0.002), and DOAC intake (OR 0.57; p = 0.038). SEC with or without THR independently predicted thromboembolic events (HR 1.74, p = 0.031 and HR 1.53, p = 0.006) and all-cause mortality (HR 1.77, p = 0.011 and HR 1.57, p = 0.002), adjusted for cardiovascular risk factors, anticoagulation, and laboratory data.
Conclusions: In AF patients undergoing TEE, SEC, often overlooked in cardioversion decisions, independently predicted thromboembolic events and mortality.
Keywords: Atrial fibrillation; Mortality; Spontaneous echo contract; Thrombus; Transesophageal echocardiography.
© 2024 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Benjamin E.J., Muntner P., Alonso A., Bittencourt M.S., Callaway C.W., Carson A.P., Chamberlain A.M., Chang A.R., Cheng S., Das S.R., et al. Heart disease and stroke statistics-2019 update: a report from the American Heart Association. Circulation. 2019;139(10):e56–e528. - PubMed
-
- Hindricks G., Potpara T., Dagres N., Arbelo E., Bax J.J., Blomstrom-Lundqvist C., Boriani G., Castella M., Dan G.A., Dilaveris P.E., et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021;42(5):373–498. - PubMed
-
- Delgado V., Di Biase L., Leung M., Romero J., Tops L.F., Casadei B., Marrouche N., Bax J.J. Structure and function of the left atrium and left atrial appendage: AF and stroke implications. J. Am. Coll. Cardiol. 2017;70(25):3157–3172. - PubMed
LinkOut - more resources
Full Text Sources
