

Predictors of glycaemic improvement in children and young adults with type 1 diabetes and very elevated HbA1c using the MiniMed 780G system
- PMID: 39831344
- PMCID: PMC11885095
- DOI: 10.1111/dom.16210
Predictors of glycaemic improvement in children and young adults with type 1 diabetes and very elevated HbA1c using the MiniMed 780G system
Abstract
Aims: This study aimed to identify key factors with the greatest influence on glycaemic outcomes in young individuals with type 1 diabetes (T1D) and very elevated glycaemia after 3 months of automated insulin delivery (AID).
Materials and methods: Data were combined and analysed from two separate and previously published studies with similar inclusion criteria assessing AID (MiniMed 780G) efficacy among young individuals naïve to AID (aged 7-25 years) with glycated haemoglobin A1c (HbA1c) ≥69 mmol/mol (≥8.5%). Univariate and multivariate linear models were performed to explore factors leading to the greatest improvements in HbA1c and time in range 3.9-10.0 mmol/L (70-180 mg/dL; TIR).
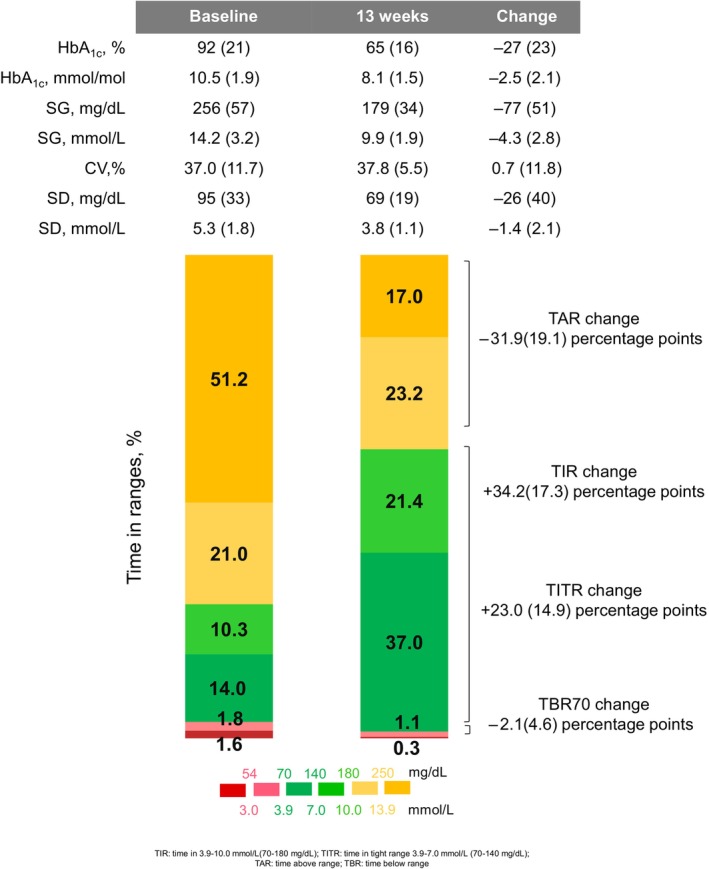
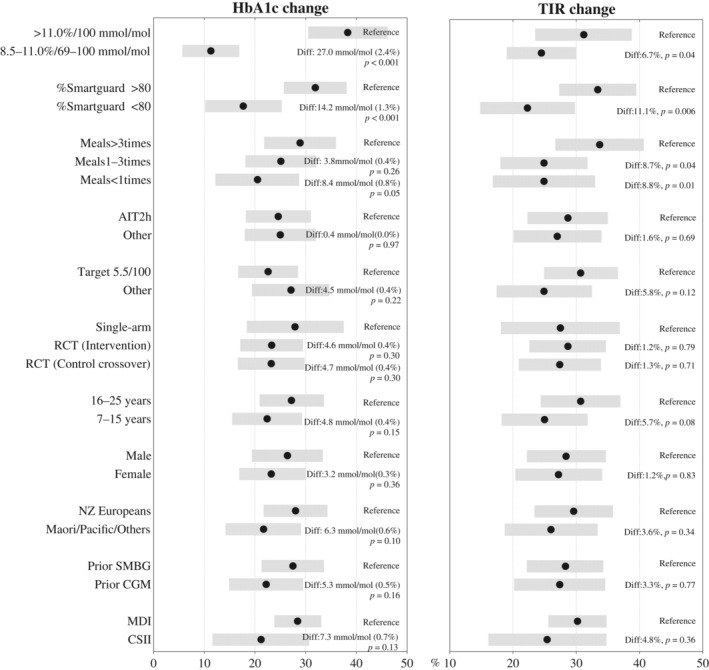
Results: A total of 99 young individuals (aged 17.3 ± 4.2 years; baseline HbA1c 92 ± 21 mmol/mol [10.6% ± 1.9%]) were included. After 3 months of AID use, HbA1c improved to 65 ± 16 mmol/mol (8.1% ± 1.5%) (-27 ± 23 mmol/mol; -2.5% ± 2.1% change), and TIR improved from 24.2% ± 13.5% to 58.4% ± 15.4% (p both <0.001). In the multivariate analysis, two key factors for both HbA1c and TIR improvement were identified: high baseline HbA1c (>100 mmol/mol [>11.0%]) and high time in automation mode (>80%), which led to decreased HbA1c by 27.0 mmol/mol (2.4%) and 14.2 mmol/mol (1.3%) and increased TIR by 6.1% and 11.1% (p all <0.05) respectively. Meal announcement frequency >3 times/day and glucose target of 5.5 mmol/L (100 mg/dL) also led to significant increases in TIR. No other factors, including age, prior use of multiple daily injection, ethnicity, gender and optimal active insulin time 2 h, contributed to statistically significant HbA1c or TIR improvement.
Conclusions: In young individuals naive to AID, those with the highest baseline HbA1c and high percentage time in automation experience the greatest benefits after initiation of AID. Sociodemographic background and carbohydrate counting adherence/knowledge should not prevent or delay access to AID technology (ACTRN12621000556842 and ACTRN12622001454763).
Keywords: automated insulin delivery; children and adolescents; type 1 diabetes mellitus.
© 2025 The Author(s). Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
This study was investigator designed and led. As above, funding for the two included studies were largely independent of Medtronic, with limited financial support from Medtronic provided for CO‐PILOT. The diabetes technology used in this study was provided by Medtronic. Medtronic was not involved in data analysis but was provided a copy of the manuscript for review before submission. B.J.W. and M.I.d.B. have received honorarium, expenses, and research funding from Medtronic. No other potential conflicts of interest relevant to this study were reported.
Figures
References
-
- Maahs DM, Hermann JM, DuBose SN, et al. Contrasting the clinical care and outcomes of 2,622 children with type 1 diabetes less than 6 years of age in the United States T1D exchange and German/Austrian DPV registries. Diabetologia. 2014;57(8):1578‐1585. - PubMed
-
- James S, Perry L, Lowe J, Harris M, Craig ME, group As . Suboptimal glycemic control in adolescents and young adults with type 1 diabetes from 2011 to 2020 across Australia and New Zealand: data from the Australasian diabetes data network registry. Pediatr Diabetes. 2022;23(6):736‐741. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
