

Lung function and onset of cardiometabolic diseases in the longitudinal Burden of Obstructive Lung Disease study
- PMID: 39832891
- PMCID: PMC11751964
- DOI: 10.1136/bmjresp-2024-002442
Lung function and onset of cardiometabolic diseases in the longitudinal Burden of Obstructive Lung Disease study
Abstract
Introduction: Previous population-based studies, mainly from high-income countries, have shown that a higher forced vital capacity (FVC) is associated with a lower risk of developing cardiometabolic diseases. The aim of this study was to assess the longitudinal association between spirometry measures and the onset of cardiometabolic diseases across sites in low-income, middle-income and high-income countries.
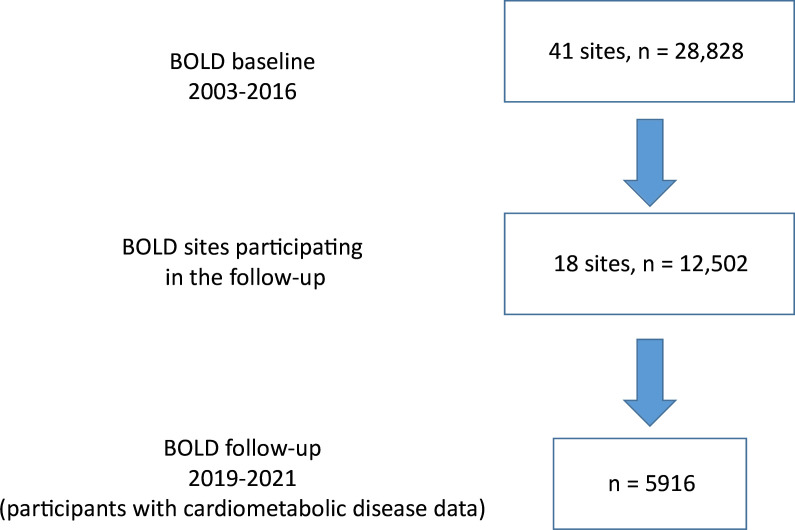
Methods: The study population comprised 5916 individuals from 15 countries participating in the Burden of Obstructive Lung Disease baseline and follow-up assessments. Postbronchodilator forced expiratory volume in 1 s (FEV1), FVC and FEV1/FVC were measured at baseline. Participants who reported having doctor-diagnosed hypertension, diabetes, heart disease and stroke at follow-up but not at baseline were considered new cases of these diseases. The association between lung function and the onset of participant-reported cardiometabolic diseases was assessed in each site using regression models, and estimates were combined using random effects meta-analysis. Models were adjusted for sex, age, smoking, body mass index and educational level.
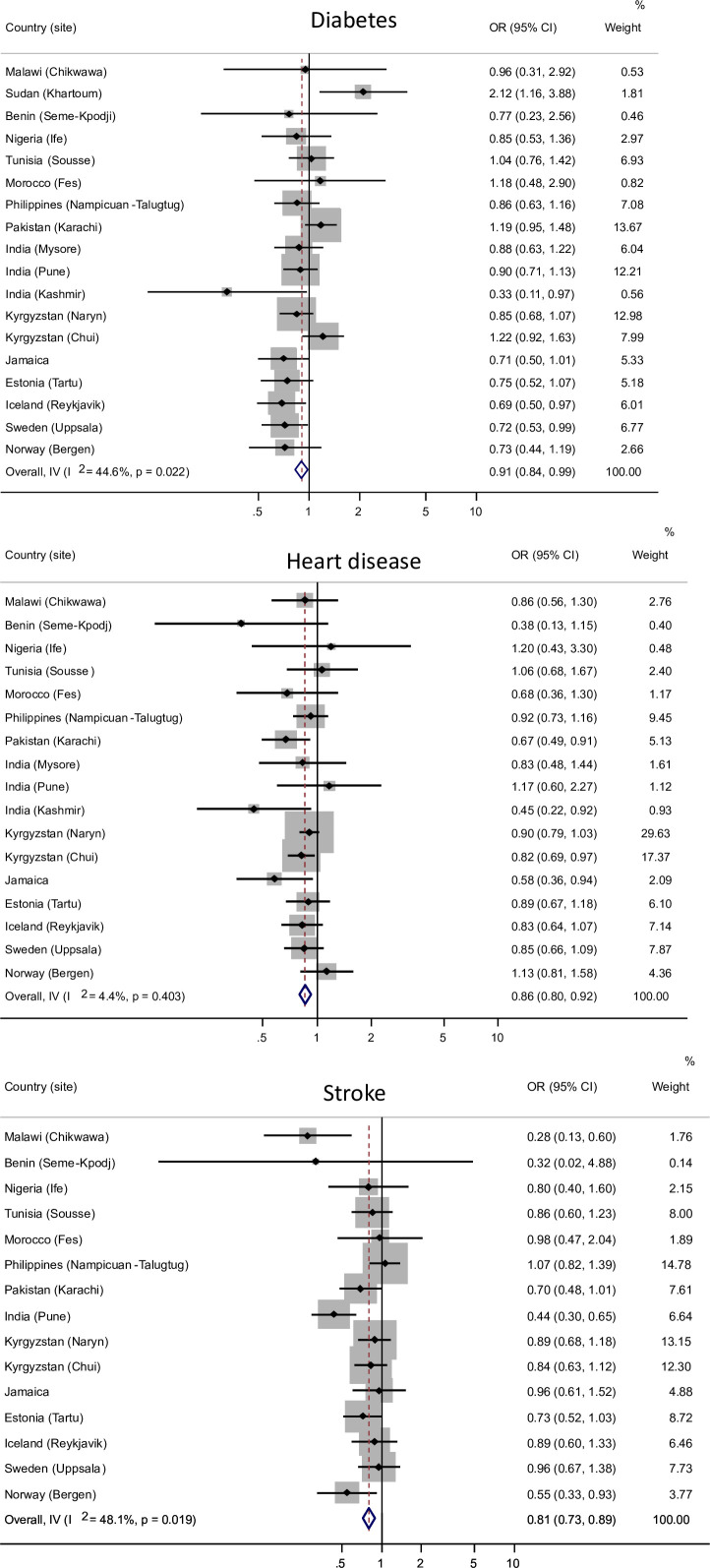
Results: Participants with greater per cent predicted FVC were less likely to have new-onset diabetes (OR per 10%=0.91, 95% CI 0.84 to 0.99), heart disease (OR per 10%=0.86, 95% CI 0.80 to 0.92) and stroke (OR per 10%=0.81, 95% CI 0.73 to 0.89) during the follow-up period (mean±SD 9.5±3.6 years). A greater percentage of FEV1 was associated with a lower risk of onset of heart disease and stroke. No significant association was found between FEV1/FVC and onset of reported cardiometabolic diseases, except for a higher risk of diabetes (OR per 10%=1.21, 95% CI 1.08 to 1.35) in participants with higher FEV1/FVC.
Conclusions: The findings of this study suggest that a low FVC is more important than a low FEV1/FVC as a risk factor for developing cardiometabolic diseases. The value of including FVC in risk score models to improve their precision in predicting the onset of cardiometabolic diseases should be explored.
Keywords: COPD epidemiology; Clinical Epidemiology; Lung Physiology.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY. Published by BMJ Group.
Conflict of interest statement
Competing interests: RN declares support from Astra Zenenca related to and the Norwegian Respiratory Society not related to the manuscript. AØR declares support from Boehringer Ingelheim and the Endowment of Timber Merchant A. Delphin and Wife unrelated to the manuscript. PGJB declares support from the Wellcome Trust related to the manuscript. AFSA declares support from the Colt Foundation not related to the manuscript. None of the other authors declare any conflicts of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources