

Machine learning validation of the AVAS classification compared to ultrasound mapping in a multicentre study
- PMID: 39833325
- PMCID: PMC11756420
- DOI: 10.1038/s41598-025-86456-3
Machine learning validation of the AVAS classification compared to ultrasound mapping in a multicentre study
Abstract
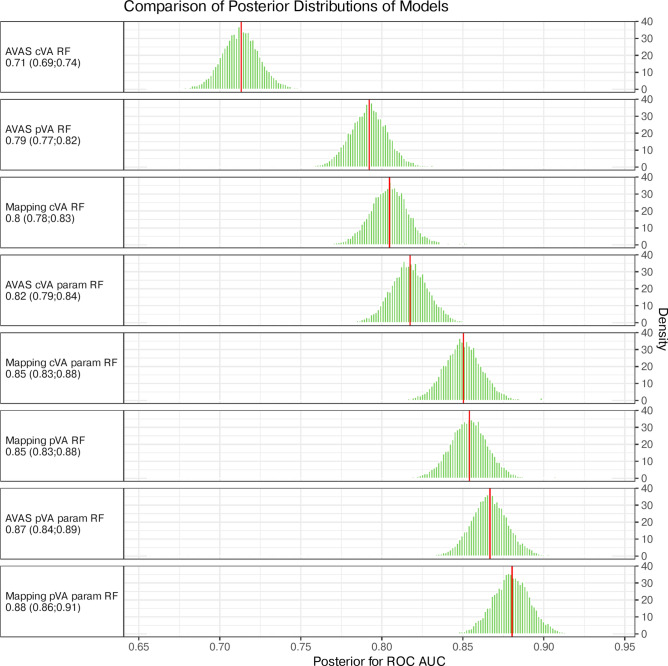
The Arteriovenous Access Stage (AVAS) classification simplifies information about suitability of vessels for vascular access (VA). It's been previously validated in a clinical study. Here, AVAS performance was tested against multiple ultrasound mapping measurements using machine learning. A prospective multicentre international study (NCT04796558) with patient recruitment from March 2021-July 2024. Demographics, risk factors, vessels parameters, types of predicted and created VA (pVA, cVA) were collected. We modelled pVA and cVA using the Random Forest algorithm. Model performance was estimated and compared using Bayesian generalized linear models. ROC AUC with 95% credible intervals was the performance metric. 1151 patients were included. ROC AUC for pVA prediction by AVAS was 0.79 (0.77;0.82) and by mapping was 0.85 (0.83;0.88). ROC AUC for cVA prediction by AVAS was 0.71 (0.69;0.74) and by mapping was 0.8 (0.78;0.83). Using AVAS with other parameters increased the ROC AUC to 0.87 for pVA (0.84;0.89) and 0.82 (0.79;0.84) for cVA. Using mapping with other parameters increased the ROC AUC to 0.88 for pVA (0.86;0.91) and 0.85 (0.83;0.88) for cVA. Multiple mapping measurements showed higher performance at VA prediction than AVAS. However, AVAS is simpler and quicker, so may be preferable for routine clinical practice.
Keywords: Arteriovenous access; Classification system; Dialysis; Mapping; Random forest; Renal replacement therapy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical approval: The study was approved by Ethics Committee of University Hospital Královské Vinohrady in Prague, Czech Republic (EK-VP/06/0/2021).
Figures



References
-
- Woo, K. T., Choong, H. L., Wong, K. S., Tan, H. B. & Chan, C. M. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int.81, 1044–1045 (2012). - PubMed
-
- Shi, B., Ying, T. & Chadban, S. J. Survival after kidney transplantation compared with ongoing dialysis for people over 70 years of age: A matched-pair analysis. Am. J. Transplant.23, 1551–1560 (2023). - PubMed
-
- Tonelli, M. et al. Systematic review: Kidney transplantation compared with dialysis in clinically relevant outcomes. Am. J. Transplant.11, 2093–2109 (2011). - PubMed
-
- Hernández, D. et al. Mortality in elderly waiting-list patients versus age-matched kidney transplant recipients: Where is the risk?. Kidney Blood Press. Res.43, 256–275. 10.1159/000487684 (2018). - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
