

Anesthesia for pregnant patients with symptomatic neurological disease: 13 years' experience from a tertiary care center
- PMID: 39833679
- PMCID: PMC11744999
- DOI: 10.1186/s12871-024-02871-5
Anesthesia for pregnant patients with symptomatic neurological disease: 13 years' experience from a tertiary care center
Abstract
Background: Improvements in diagnostics and clinical care have allowed more women of childbearing age, suffering from neurological diseases, to safely have pregnancy, reducing peripartum complications. However, these patients remain at risk and are a constant challenge for anesthesiologists in the delivery room.
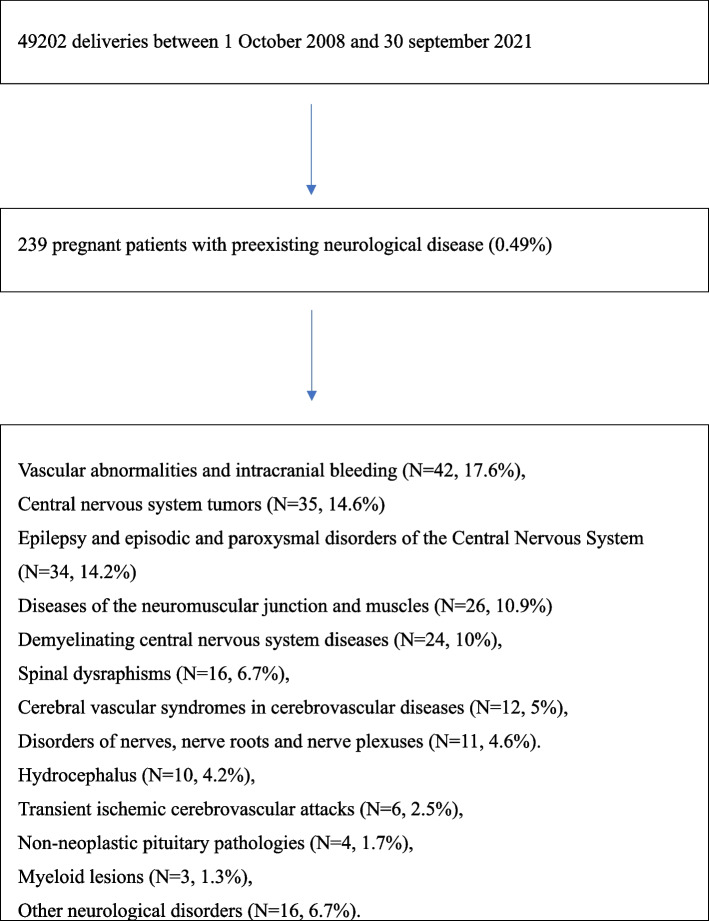
Methods: To assess the type of anesthesiologic management performed for delivery in obstetric patients with preexisting neurological disease and who reported significant neurological symptoms during pregnancy, a retrospective observational study was carried out between 1 October 2008 and 30 September 2021.
Results: Data from 49,202 pregnant women were assessed over 13 years; 239 pregnant women with a diagnosis of preexisting neurological disease and who reported significant neurological symptoms during pregnancy were identified (prevalence 0.49%). The main neurological disorders that affected pregnant women included vascular abnormalities and intracranial bleeding (N = 42, 17.6%), central nervous system tumors (N = 35, 14.6%), epilepsy and episodic and paroxysmal disorders of the central nervous system (N = 34, 14.2%), diseases of the neuromuscular junction and muscles (N = 26, 10.9%), demyelinating central nervous system diseases (N = 24, 10%). A total of 234 (97.9%) pregnant women with neurological disorders and significant neurological symptoms underwent cesarean section: 192 (80.3% of the total cesarean sections) were elective, 39 (16.3%) were urgent type 2 and 3; 3 (1.2%) were emergency cesarean sections. General anesthesia was administered to 73 patients (30.5%), while 166 patients (69.5%) were managed with neuraxial techniques. 2 patients who had had neuraxial block reported worsening neurological symptoms that required a change in medical therapy. Postoperative multiparameter monitoring was performed for less than 24 h in the recovery room for 226 patients (94.6%). 3 patients (1.2%) were observed with multiparameter monitoring in the post-anesthesia care unit (PACU) for more than 24 hours; 10 patients (4.2%) were moved to the postoperative intensive care unit (ICU). The median hospitalization duration was 4 days (with an interquartile difference of 3-6 days).
Conclusions: In our experience, when neuraxial anesthesia was feasible, it proved to be a safe option for pregnant patients with symptomatic neurological disease, resulting in uncommon maternal complications.
Keywords: Cesarean section; Neurological disease; Neuromuscular disease; Obstetric anesthesia; Pregnancy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This observational retrospective study received approval for data extraction and processing from the Policlinico A. Gemelli Ethics Committee, without ad hoc consent from the enrolled patients (protocol ID 3741). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- van den Bersselaar LR, Heytens L, Silva HCA, Reimann J, Tasca G, Díaz-Cambronero Ó, Løkken N, Hellblom A, Hopkins PM, Rueffert H, Bastian B, Vilchez JJ, Gillies R, Johannsen S, Veyckemans F, Muenster T, Klein A, Litman R, Jungbluth H, Riazi S, Voermans NC, Snoeck MMJ. European Neuromuscular Centre consensus statement on anaesthesia in patients with neuromuscular disorders. Eur J Neurol. 2022;29(12):3486–507. - DOI - PMC - PubMed
-
- MBRRACE-UK Saving Lives, Improving Mothers’ Care report for 2023. https://www.npeu.ox.ac.uk/assets/downloads/mbrrace-uk/reports/maternal-r.... - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
