

CMR assessment of epicardial edipose tissue in relation to myocardial inflammation and fibrosis in patients with new-onset atrial arrhythmias after STEMI
- PMID: 39833688
- PMCID: PMC11748530
- DOI: 10.1186/s12872-025-04486-1
CMR assessment of epicardial edipose tissue in relation to myocardial inflammation and fibrosis in patients with new-onset atrial arrhythmias after STEMI
Abstract
Background: Previous studies have shown that epicardial edipose tissue(EAT) appears to be associated with myocardial inflammation and fibrosis, but this is not clear in patients with new-onset atrial arrhythmias after STEMI. The present study focused on using CMR to assess the association of epicardial fat with myocardial inflammation and fibrosis and its predictive value in patients with new-onset atrial arrhythmias after STEMI.
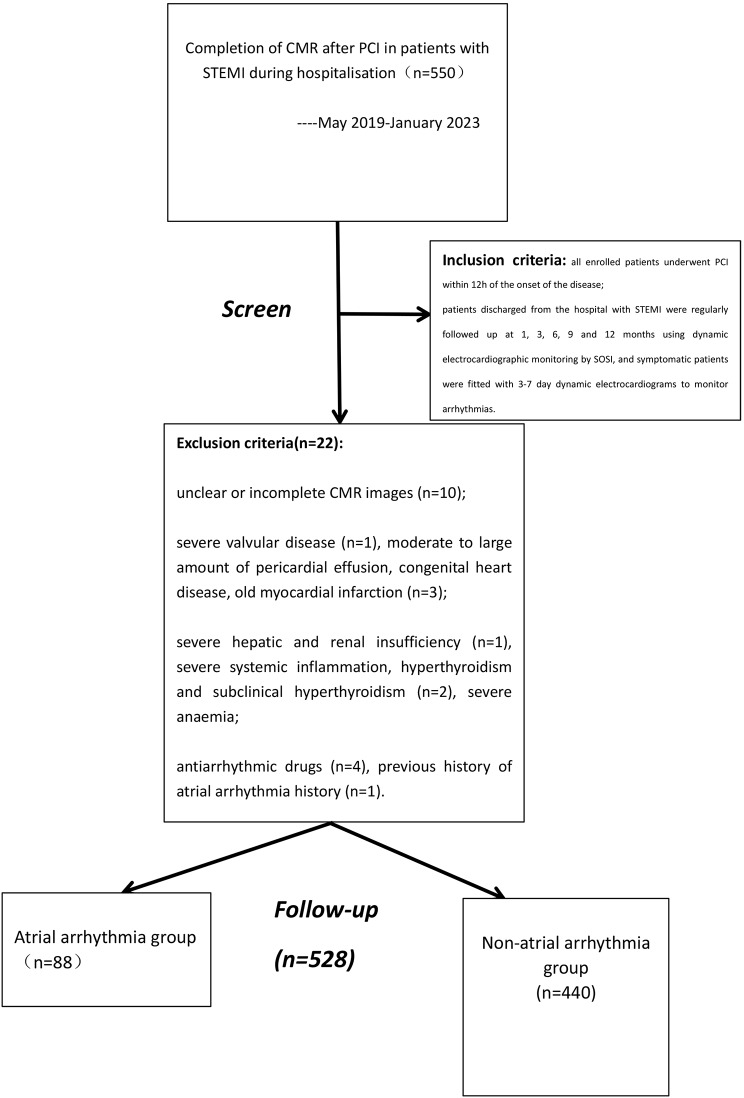
Methods: This was a single-centre, retrospective study. We consecutively selected patients who completed CMR during their hospitalisation for PCI after STEMI from May 2019-January 2023, and then underwent regular follow-up, grouped by the presence or absence of new atrial arrhythmias, and enrolled patients were divided into atrial arrhythmia and non-atrial arrhythmia groups.
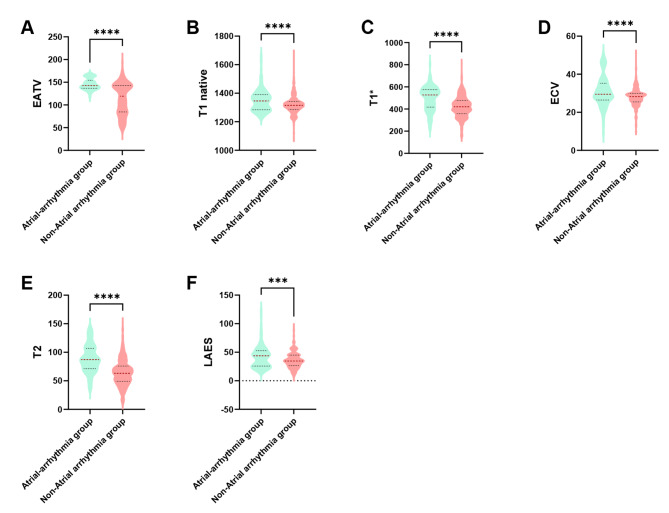
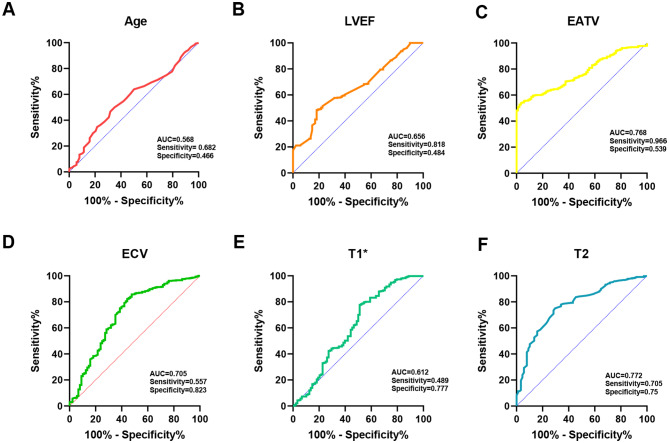
Results: In the atrial arrhythmia group, age, heart rate, Peak hs-TnT, PeakNT-proBNP, EATV, LAES, LAED, T1 native, T1*, ECV, and T2 were higher than those in the non-atrial arrhythmia group, and LVEF was lower than those in the non-atrial arrhythmia group. EATV showed a positive and significant correlation with T1native, T1*, ECV, and T2. (T1 native: r = 0.476,p < 0.001; ECV: r = 0.529,p < 0.001; T1*: r = 0.467,p < 0.001; T2: r = 0.538,p < 0.001). Multifactorial logistic regression analysis showed age, LVEF, EATV, T1*,ECV, T2 as independent risk factors for atrial arrhythmia. (p < 0.05) ROC analysis showed that the AUC for age was 0.568; AUC for LVEF was 0.656; AUC for EATV was 0.768; AUC for ECV was 0.705; AUC for T1* was 0.612; and AUC for T2 was 0.772.
Conclusion: In patients with STEMI, EAT is associated with myocardial inflammation, fibrosis. Age, LVEF, EATV, T1*,ECV, T2 are independent risk factors for new onset atrial arrhythmias and have good predictive value.
Keywords: Atrial arrhythmia; CMR; ECV; Epicardial adipose tissue; T1mapping; T2mapping.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The requirement for signed written consent was waived owing to no risk to the patient in accordance with the relevant IRB regulatory guidelines. This study was approved by the Ethics Committee of Xuzhou Medical University Affiliated Hospital, and complied with the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Correlation of epicardial adipose tissue with microvascular obstruction and its effect on new-onset atrial arrhythmias after PCI in STEMI patients.Sci Rep. 2025 Feb 11;15(1):5052. doi: 10.1038/s41598-025-89568-y. Sci Rep. 2025. PMID: 39934305 Free PMC article.
-
Correlation of epicardial adipose tissue and inflammatory indices in patients with STEMI and implications for atrial arrhythmias.Int J Cardiol. 2024 Jul 1;406:132016. doi: 10.1016/j.ijcard.2024.132016. Epub 2024 Apr 8. Int J Cardiol. 2024. PMID: 38599466
-
Epicardial Adipose Tissue and Heterogeneity Parameters Combined with Inflammatory Cells to Predict the Value of Heart Failure with Preserved Ejection Fraction Patients Post Myocardial Infarction.Cardiovasc Diabetol. 2025 May 3;24(1):192. doi: 10.1186/s12933-025-02720-w. Cardiovasc Diabetol. 2025. PMID: 40319313 Free PMC article.
-
Association Between Extracellular Volume Assessed by Cardiac MRI and New-Onset Atrial Fibrillation in Patients With ST-Segment Elevation Myocardial Infarction.Korean J Radiol. 2025 Jun;26(6):546-556. doi: 10.3348/kjr.2025.0070. Korean J Radiol. 2025. PMID: 40432261 Free PMC article.
-
Epicardial adipose tissue as a mediator of cardiac arrhythmias.Am J Physiol Heart Circ Physiol. 2022 Feb 1;322(2):H129-H144. doi: 10.1152/ajpheart.00565.2021. Epub 2021 Dec 10. Am J Physiol Heart Circ Physiol. 2022. PMID: 34890279 Free PMC article. Review.
Cited by
-
Association of epicardial fat volume with the severity of coronary artery disease: a preliminary study on risk prediction of obstructive coronary heart disease.BMC Cardiovasc Disord. 2025 Apr 17;25(1):293. doi: 10.1186/s12872-025-04743-3. BMC Cardiovasc Disord. 2025. PMID: 40247180 Free PMC article.
-
Clinical prediction study on the risk of atrial fibrillation in hypertensive patients based on metabolism, inflammation, and gender differences.Sci Rep. 2025 Apr 12;15(1):12678. doi: 10.1038/s41598-025-97965-6. Sci Rep. 2025. PMID: 40221620 Free PMC article.
References
-
- Bhatt DL, Lopes RD, Harrington RA. Diagnosis and treatment of Acute Coronary syndromes: a review. JAMA. 2022;327(7):662–75. - PubMed
-
- Goudis CA, Vasileiadis IE, Liu T. Epicardial adipose tissue and atrial fibrillation: pathophysiological mechanisms, clinical implications, and potential therapies. Curr Med Res Opin. 2018;34(11):1933–43. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
