

Impact of mild hypothermic circulatory arrest on surgical outcomes in acute type a aortic dissection patients: a single-centre study
- PMID: 39833714
- PMCID: PMC11748564
- DOI: 10.1186/s12872-024-04443-4
Impact of mild hypothermic circulatory arrest on surgical outcomes in acute type a aortic dissection patients: a single-centre study
Abstract
Background: As hypothermic circulatory arrest (HCA) is being more frequently induced in patients undergoing aortic arch surgery, its safety at different degrees has become a crucial area of study. The aim of this study was to assess the surgical outcomes of mild hypothermic circulatory arrest (MI-HCA) during aortic arch surgery.
Methods: Acute type A aortic dissection (ATAAD) patients who underwent total arch replacement (TAR) and frozen elephant trunk (FET) surgery between January 2014 and December 2023 were enrolled in this study. The patients were divided into two groups according to the minimum nasopharyngeal temperature: the moderate hypothermic circulatory arrest (MHCA) group (20-28 °C) and the MI-HCA group (> 28 °C). The inverse probability of treatment weighting (IPTW) was used to balance differences in the baseline characteristics. Perioperative variables were analysed via pairwise comparisons, multivariable logistic regression, and subgroup forest plots to assess the impact of MI-HCA on surgical outcomes.
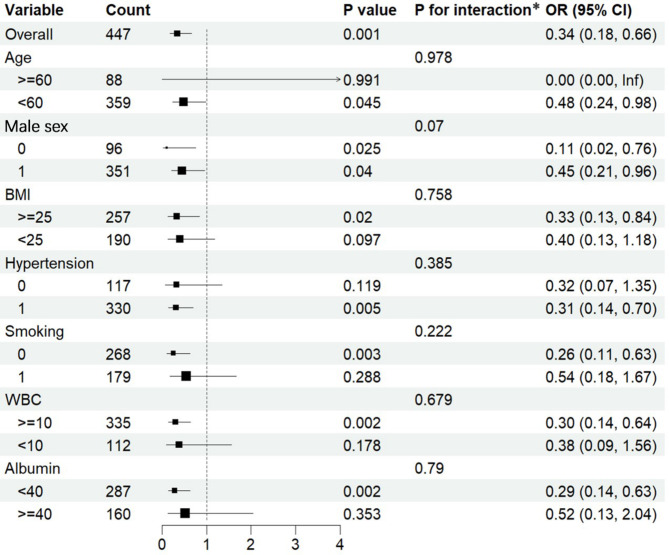
Results: A total of 447 patients were included in this study, and the mean minimum nasopharyngeal temperature was 24.80 (23.98, 27.30) °C in the MHCA group and 30.10 (29.80, 30.70) °C in the MI-HCA group. The incidence of acute kidney injury (AKI) in the MI-HCA group was lower than that in the MHCA group (52% vs. 78%, p < 0.01). In the multivariable logistic regression analysis, MI-HCA was identified as an independent protective factor for AKI (OR = 0.354, 95% CI 0.177-0.689; p = 0.003). Additionally, compared with MHCA, MI-HCA was not associated with an increased incidence of stroke, spinal cord injury, or in-hospital mortality. After IPTW, the preoperative and intraoperative data of the patients were balanced, and the incidence of AKI in the MI-HCA group was still lower than that in the MHCA group (83.26% vs. 53.61%, p = 0.004). The subgroup forest plot also demonstrated that MI-HCA was a protective factor for postoperative AKI.
Conclusions: The surgical outcomes of MI-HCA in ATAAD patients were satisfactory. Compared with MHCA, MI-HCA provided sufficient protection for distal organs, the brain, and the spinal cord, with a significantly lower incidence of AKI. These results indicate that MI-HCA could be a better approach for ATAAD surgery.
Keywords: Acute kidney injury; Acute type a aortic dissection; Inverse probability of treatment weighting; Mild hypothermic circulatory arrest; Subgroup forest plot; Surgical outcomes.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was reviewed and approved by the ethics committee of the Second Xiangya Hospital of Central South University, and the approval number is LYF2023113. All patients provided written informed consent for the use of access to their retrospective data and samples in research. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests. Clinical trial number: Not applicable.
Figures

Similar articles
-
Moderate and deep hypothermic circulatory arrest has a comparable effect on acute kidney injury after total arch replacement with frozen elephant trunk procedure in type A aortic dissection.Interact Cardiovasc Thorac Surg. 2019 Jul 1;29(1):130-136. doi: 10.1093/icvts/ivz092. Interact Cardiovasc Thorac Surg. 2019. PMID: 30977797
-
Risk factors for acute kidney injury in aortic arch surgery with selective cerebral perfusion and mild hypothermic lower body circulatory arrest.Interact Cardiovasc Thorac Surg. 2014 Dec;19(6):955-61. doi: 10.1093/icvts/ivu241. Epub 2014 Jul 15. Interact Cardiovasc Thorac Surg. 2014. PMID: 25028074
-
Moderate Hypothermic Circulatory Arrest with Antegrade Cerebral Perfusion for Rapid Total Arch Replacement in Acute Type A Aortic Dissection.Thorac Cardiovasc Surg. 2016 Mar;64(2):124-32. doi: 10.1055/s-0035-1555752. Epub 2015 Jul 15. Thorac Cardiovasc Surg. 2016. PMID: 26177224
-
Optimal temperature management in aortic arch surgery: A systematic review and network meta-analysis.J Card Surg. 2022 Dec;37(12):5379-5387. doi: 10.1111/jocs.17206. Epub 2022 Nov 15. J Card Surg. 2022. PMID: 36378895 Free PMC article.
-
A Meta-Analysis of Total Arch Replacement With Frozen Elephant Trunk in Acute Type A Aortic Dissection.Vasc Endovascular Surg. 2016 Jan;50(1):33-46. doi: 10.1177/1538574415624767. Epub 2016 Jan 14. Vasc Endovascular Surg. 2016. PMID: 26767803 Review.
References
-
- Evangelista A, Isselbacher EM, Bossone E, Gleason TG, Eusanio MD, Sechtem U, Ehrlich MP, Trimarchi S, Braverman AC, Myrmel T, et al. Insights from the International Registry of Acute Aortic dissection: a 20-Year experience of collaborative clinical research. Circulation. 2018;137(17):1846–60. - PubMed
-
- Sef D, Thet MS, Acharya M, Tyson N, Hadjinikolaou L, Mariscalco G, Oo A, Benedetto U, Luthra S. Aortic arch replacement in patients with previous repair of acute aortic dissection: a systematic review and meta-analysis. Eur J Cardiothorac Surg. 2024;66(5). - PubMed
-
- Malaisrie SC, Szeto WY, Halas M, Girardi LN, Coselli JS, Sundt TM 3rd, Chen EP, Fischbein MP, Gleason TG, Okita Y, et al. 2021 the American Association for Thoracic Surgery expert consensus document: Surgical treatment of acute type a aortic dissection. J Thorac Cardiovasc Surg. 2021;162(3):735–e758732. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
