

Mixed vulnerabilities: the biological risk of high parity is aggravated by emergency referral in Benin, Malawi, Tanzania and Uganda
- PMID: 39833887
- PMCID: PMC11744807
- DOI: 10.1186/s12939-025-02379-5
Mixed vulnerabilities: the biological risk of high parity is aggravated by emergency referral in Benin, Malawi, Tanzania and Uganda
Abstract
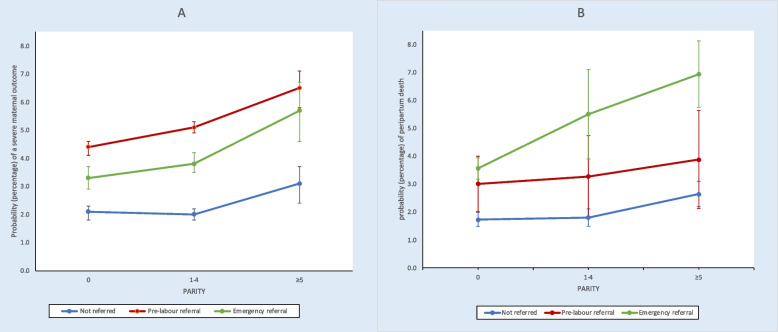
Identification of interacting vulnerabilities is essential to reduce maternal and perinatal mortality in sub-Saharan Africa (SSA). High parity (≥ 5 previous births) is an underemphasized biological vulnerability linked to poverty and affecting a sizeable proportion of SSA births. Despite increased risk, high parity women rarely use hospitals for childbirth. We assessed whether emergency referral during childbirth was associated with adverse events in high parity women in hospitals in Benin, Malawi, Tanzania and Uganda. We used e-registry data collected in 16 hospitals included in the Action Leveraging Evidence to Reduce perinatal morbidity and morTality (ALERT) trial. Main outcomes were severe maternal outcomes and in-facility peripartum death (fresh stillbirth or very early neonatal death). Main exposure was parity; emergency (in-labour) referral was included as effect modifier with potential confounders. We used multivariable logistic regression including parity/referral interaction and post-regression margins analysis. Among 80,663 births, 4,742 (5.9%) were to high parity women. One third reached hospital following emergency referral. Severe maternal outcomes and peripartum mortality were over 2.5-fold higher in high parity women with emergency referral compared to the lowest risk group. To avert these adverse events, emergency referral must be avoided by ensuring high parity women give birth in hospitals. Trial registration Pan African Clinical Trial Registry ( www.pactr.org ): PACTR202006793783148. Registered on 17th June 2020.
Keywords: Childbirth; Emergency referral; Fresh stillbirths; High parity; Hospitals; Intrapartum care; Maternal health; Perinatal health; Sub-Saharan Africa; Very early neonatal mortality; Vulnerability.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval for ALERT was obtained from institutional review boards in Benin, Malawi, Tanzania, Uganda, Sweden, and Belgium, as follows: 1. Sweden: Etikprövningsmyndigheten— (Dnr 2020–01587). 2. Benin: Comité National d’Ethique pour la Recherche en Santé, Cotonou, Bénin—(N∘44 du 21/12/2020). 3. Malawi: College of Medicine Research and Ethics Committee (COMREC)—(COMREC P.04/20/3038). 4. Tanzania: Muhimbili University of Health and Allied Sciences (MUHAS), Senate Research and Publication Committee, Tanzania (MUHAS-REC-04–2020-118); the Aga Khan University Ethical Review Committee, Tanzania (AKU/2019/044/fb); and National Human Research Ethics Committee (NatHREC), Tanzania (NIMR/HQ/R.8a/Vol.IX/3493). 5. Uganda: Makerere University School of Public Health Research and Ethics committee (Protocol 808) and Uganda National Council for Science and Technology— (HS1324ES). 6. Belgium: The Institutional Review Board at the Institute of Tropical Medicine Antwerp and the Ethics Committee at the University Hospital Antwerp, Belgium—(ITG 1375/20.B3002020000116). Ethics approval from all countries exempted the study from informed individual consent from women, as data would be de-identified before incorporation into the e-registry. All study procedures were in accordance with national ethical standards on human experimentation and with the Helsinki Declaration. Consent for publication: Not applicable. Competing interests: TvdA is part of the editorial board of BMC Pregnancy and Childbirth. There are no other competing interests.
Figures
Similar articles
-
Action leveraging evidence to reduce perinatal mortality and morbidity (ALERT): study protocol for a stepped-wedge cluster-randomised trial in Benin, Malawi, Tanzania and Uganda.BMC Health Serv Res. 2021 Dec 11;21(1):1324. doi: 10.1186/s12913-021-07155-z. BMC Health Serv Res. 2021. PMID: 34895216 Free PMC article. Clinical Trial.
-
Birth asphyxia and its association with grand multiparity and referral among hospital births: A prospective cross-sectional study in Benin, Malawi, Tanzania and Uganda.Acta Obstet Gynecol Scand. 2024 Mar;103(3):590-601. doi: 10.1111/aogs.14754. Epub 2024 Jan 6. Acta Obstet Gynecol Scand. 2024. PMID: 38183308 Free PMC article.
-
Assessment of midwifery care providers intrapartum care competencies, in four sub-Saharan countries: a mixed-method study protocol.Reprod Health. 2021 Feb 27;18(1):50. doi: 10.1186/s12978-021-01109-8. Reprod Health. 2021. PMID: 33639966 Free PMC article.
-
Death audits and reviews for reducing maternal, perinatal and child mortality.Cochrane Database Syst Rev. 2020 Mar 25;3(3):CD012982. doi: 10.1002/14651858.CD012982.pub2. Cochrane Database Syst Rev. 2020. PMID: 32212268 Free PMC article.
-
Assessing pregnancy and neonatal outcomes in Malawi, South Africa, Uganda, and Zimbabwe: Results from a systematic chart review.PLoS One. 2021 Mar 31;16(3):e0248423. doi: 10.1371/journal.pone.0248423. eCollection 2021. PLoS One. 2021. PMID: 33788867 Free PMC article.
References
-
- UNICEF. Data by topic and country. Available from: https://data.unicef.org/resources/. Accessed 22 Oct 2023.
-
- Trends in maternal mortality 2000 to 2020: estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division. Geneva: World Health Organization; 2023. Available from https://www.who.int/publications/i/item/9789240068759.
-
- DHS program - Demographic and Health Surveys. The DHS program Available from: https://dhsprogram.com/. Accessed 22 Oct 2023.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
