

The Diagnostic Value of Bile Acids and Amino Acids in Differentiating Acute Coronary Syndromes
- PMID: 39834909
- PMCID: PMC11742763
- DOI: 10.2147/IJGM.S499046
The Diagnostic Value of Bile Acids and Amino Acids in Differentiating Acute Coronary Syndromes
Abstract
Purpose: Acute coronary syndrome (ACS), comprising unstable angina and acute myocardial infarction, is the most dangerous and fatal form of coronary heart disease. This study evaluates serum bile acids (BAs) and amino acids (AAs) as potential predictors of AMI in UA patients.
Patients and methods: A total of 72 Non-Coronary Artery Disease (NCAD) patients, 157 UA patients, and 79 AMI patients were analyzed. Liquid chromatography-tandem mass spectrometry (LC-MS/MS) measured 15 bile acids and 19 amino acids. The data was split into training and validation sets (7:3). Univariate and multivariate analyses were performed. Diagnostic value and clinical benefits were assessed using receiver operating characteristic (ROC) curves, decision curve analysis, and metrics such as the area under the curve (AUC), integrated discrimination improvement (IDI), and net reclassification improvement (NRI).
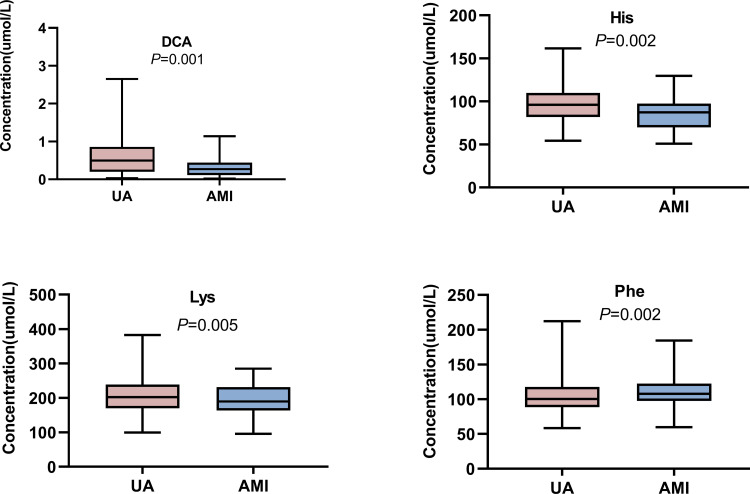
Results: Orthogonal partial least squares discriminant analysis (OPLS-DA) of serum BAs and AAs effectively differentiated NCAD, UA, and AMI groups. The differences in serum BA and AA profiles between UA and AMI patients were primarily driven by four metabolites: deoxycholic acid (DCA), histidine (His), lysine (Lys), and phenylalanine (Phe). Together, they had an AUC of 0.830 (0.768 in the validation cohort) for predicting AMI in UA patients. After adjusting for multiple confounding factors, DCA, His, Lys, and Phe were independent predictors distinguishing UA from AMI. The results of AUC, IDI, and NRI showed that adding these four biomarkers to a model with clinical variables significantly improved predictive value, which was confirmed in the validation cohort.
Conclusion: These findings highlight the association of DCA, His, Lys, and Phe with AMI, suggesting their potential role in AMI pathogenesis.
Keywords: acute myocardial infarction; amino acid; bile acid; metabolomics; unstable angina.
© 2025 Yu et al.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


Similar articles
-
Association of Serum Bile Acid and Unsaturated Fatty Acid Profiles with the Risk of Diabetic Retinopathy in Type 2 Diabetic Patients.Diabetes Metab Syndr Obes. 2023 Jul 13;16:2117-2128. doi: 10.2147/DMSO.S411522. eCollection 2023. Diabetes Metab Syndr Obes. 2023. PMID: 37465650 Free PMC article.
-
Improved Risk Prediction of Acute Myocardial Infarction in Patients With Stable Coronary Artery Disease Using an Amino Acid-Assisted Model.Cardiovasc Ther. 2024 Aug 30;2024:9935805. doi: 10.1155/2024/9935805. eCollection 2024. Cardiovasc Ther. 2024. PMID: 39742009 Free PMC article.
-
Comprehensive Metabolomic Characterization of Coronary Artery Diseases.J Am Coll Cardiol. 2016 Sep 20;68(12):1281-93. doi: 10.1016/j.jacc.2016.06.044. J Am Coll Cardiol. 2016. PMID: 27634119
-
Multinomial machine learning identifies independent biomarkers by integrated metabolic analysis of acute coronary syndrome.Sci Rep. 2023 Nov 23;13(1):20535. doi: 10.1038/s41598-023-47783-5. Sci Rep. 2023. PMID: 37996510 Free PMC article.
-
[The significance of a 4,183 Da peptide of dermcidin protein in the early diagnosis and differential diagnosis of acute coronary syndrome].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015 Dec;27(12):970-4. doi: 10.3760/cma.j.issn.2095-4352.2015.12.006. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015. PMID: 27318339 Chinese.
References
-
- Barstow C, Rice M, McDivitt JD. Acute coronary syndrome: diagnostic evaluation. Am Family Phys. 2017;95(3):170–177. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
