

Phosphate binder in dialysis: a cross-sectional study of patients' adherence and pill burden
- PMID: 39835716
- PMCID: PMC11748762
- DOI: 10.1590/2175-8239-JBN-2024-0075en
Phosphate binder in dialysis: a cross-sectional study of patients' adherence and pill burden
Abstract
Introduction: Phosphate (P) binders are among the most common medications prescribed to control P levels in patients with chronic kidney disease on dialysis. There is still a paucity of data on adherence to P binders with no comparison between dialysis modalities.
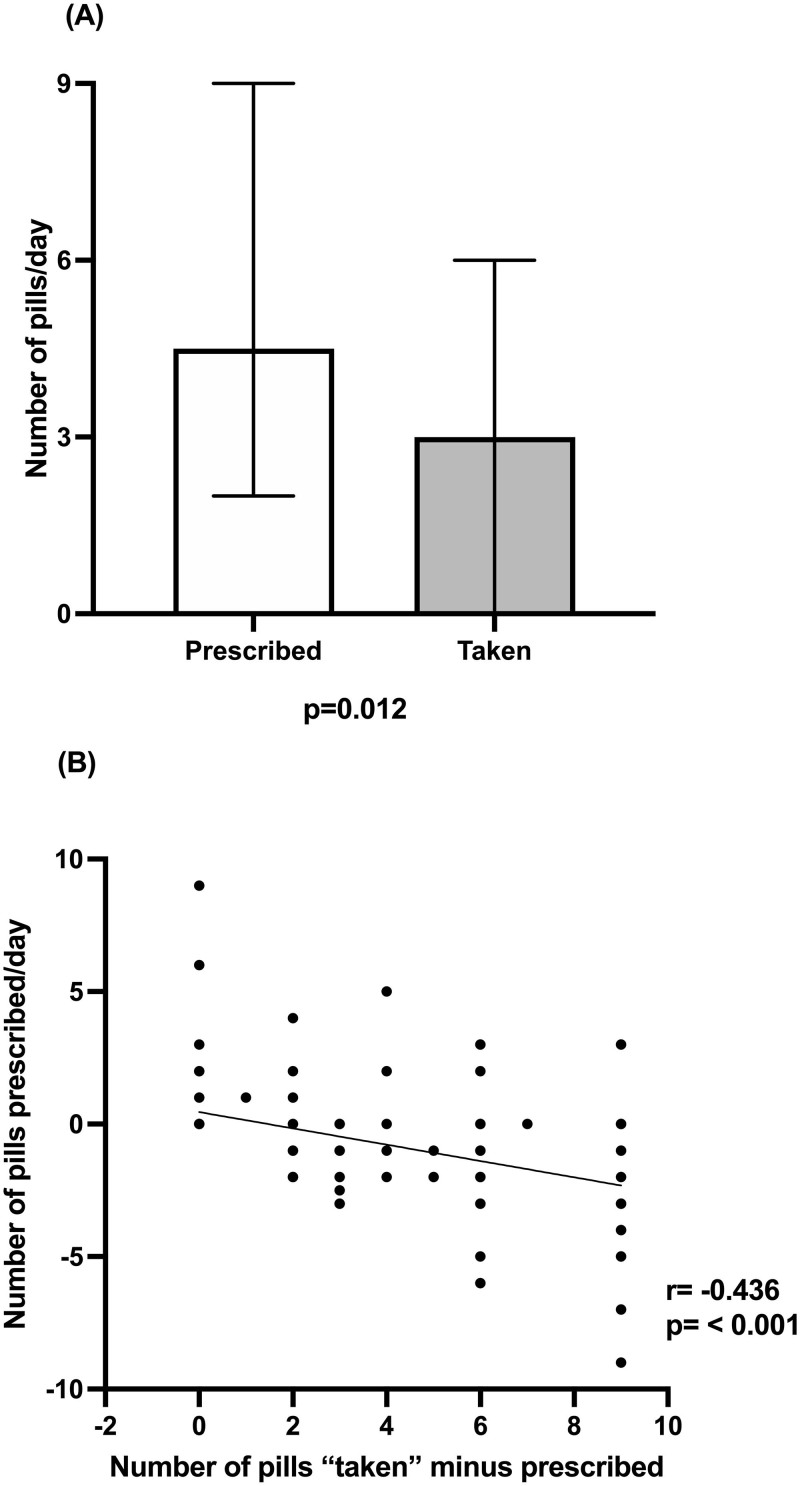
Methods: We accessed factors associated with P binder adherence among patients on dialysis in an academic hospital. Adherence was calculated as the ratio between the number of pills taken per day as reported and the prescribed number of pills. Patients were considered non-adherent if adherence was at least 20% less or 30% more than prescribed.
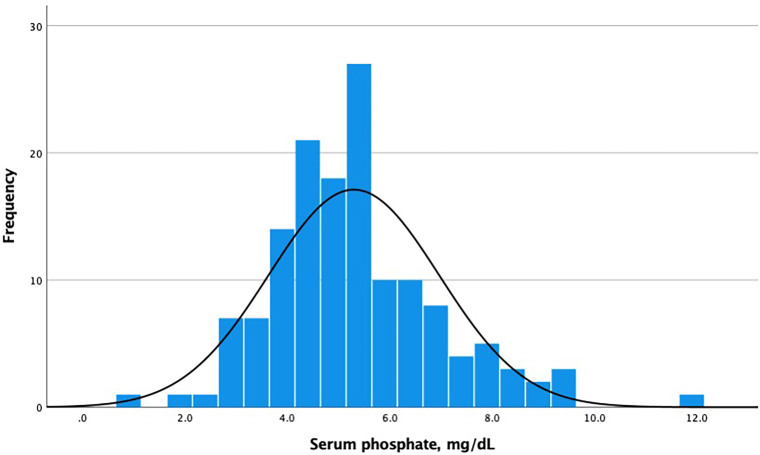
Results: Patients (N = 137) were young, mostly women, and on dialysis for a median time of 53 months. Sevelamer and calcium carbonate were prescribed as P binders to 70.8% and 10.2% of patients, respectively, with no difference across dialysis modalities (p = 0.839). P correlated with the number of pills prescribed (r = 0.368, p = 0.001) and the number of pills taken per day (r = 0.275, p = 0.001). Hyperphosphatemia was found in 52 patients (36.4%). Adherence to Ca carbonate and sevelamer was 100% and 68.4%, respectively. Non-adherent patients were women, younger, with higher serum albumin and urea, and lower serum calcium. Logistic regression showed that female sex (HR 3.30, 95% CI: 1.39-7.84, p = 0.007) and hemodialysis vs. peritoneal dialysis (HR 4.55, 95%, CI: 1.26-16.39, p = 0.021) remained independently associated with a non-adherence behavior.
Conclusions: The current study suggests that strategies to increase adherence should be implemented. Whether phosphate binder adherence is associated with better outcomes deserves further investigation.
Introdução:: Quelantes de fosfato (P) estão entre os medicamentos mais comumente prescritos para controlar níveis de P em pacientes com DRC em diálise. Ainda há escassez de dados sobre adesão aos quelantes de P, sem comparações entre modalidades dialíticas.
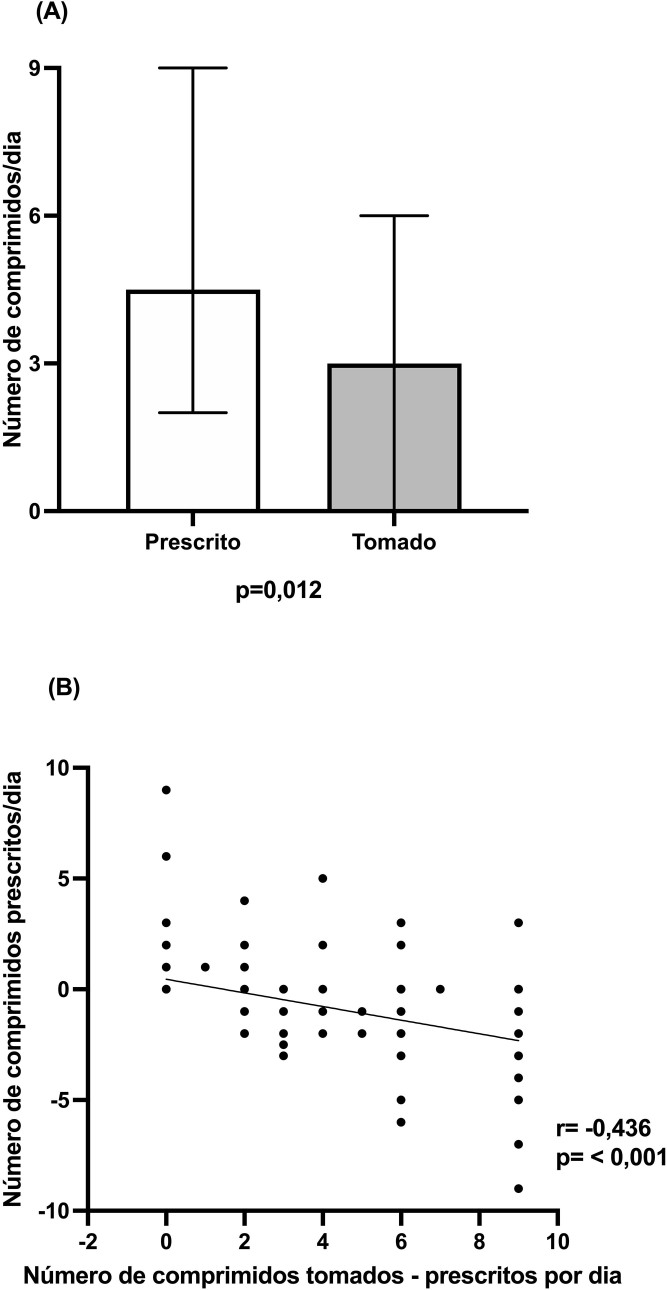
Métodos:: Acessamos fatores associados à adesão ao quelante de P entre pacientes em diálise em um hospital universitário. A adesão foi calculada como a razão entre número de comprimidos tomados por dia, conforme relatado, e número de comprimidos prescritos. Pacientes foram considerados não aderentes se a adesão fosse ao menos 20% menor ou 30% maior do que o prescrito.
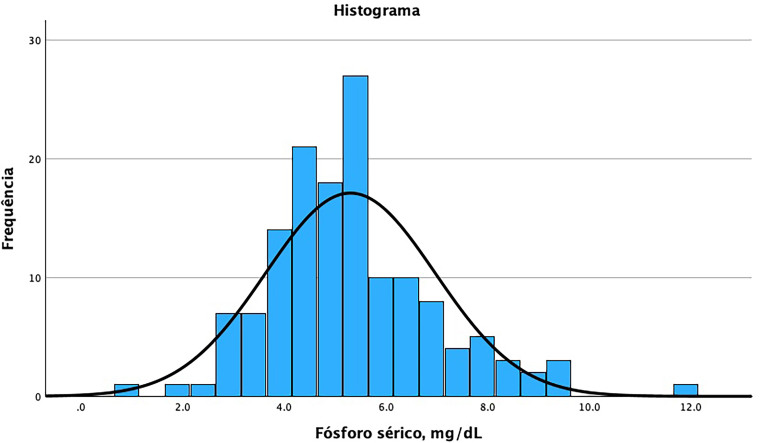
Resultados:: Os pacientes (N = 137) eram jovens, predominantemente mulheres, em diálise por um período mediano de 53 meses. Sevelamer e carbonato de cálcio foram prescritos como quelantes de P para 70,8% e 10,2% dos pacientes, respectivamente, sem diferença entre modalidades dialíticas (p = 0,839). P correlacionou-se com número de comprimidos prescritos (r = 0,368; p = 0,001) e número de comprimidos tomados por dia (r = 0,275; p = 0,001). Encontramos hiperfosfatemia em 52 pacientes (36,4%). A adesão ao carbonato de Ca e sevelamer foi de 100% e 68,4%, respectivamente. Pacientes não aderentes eram mulheres, mais jovens, com albumina e ureia séricas mais elevadas e menor cálcio sérico. A regressão logística mostrou que sexo feminino (HR 3,30; IC 95%: 1,39–7,84; p = 0,007) e hemodiálise vs. diálise peritoneal (HR 4,55; IC 95%: 1,26–16,39; p = 0,021) permaneceram independentemente associados ao comportamento de não adesão.
Conclusão:: O presente estudo sugere que estratégias para aumentar a adesão devem ser implementadas. A relação entre adesão ao quelante de fosfato e melhores desfechos merece investigação mais aprofundada.
Conflict of interest statement
None.
Figures
Similar articles
-
The economic impact of improving phosphate binder therapy adherence and attainment of guideline phosphorus goals in hemodialysis patients: a Medicare cost-offset model.Adv Ther. 2014 Dec;31(12):1272-86. doi: 10.1007/s12325-014-0170-4. Epub 2014 Dec 6. Adv Ther. 2014. PMID: 25479935
-
Intensive Hemodialysis, Mineral and Bone Disorder, and Phosphate Binder Use.Am J Kidney Dis. 2016 Nov;68(5S1):S24-S32. doi: 10.1053/j.ajkd.2016.05.024. Am J Kidney Dis. 2016. PMID: 27772640 Review.
-
Initiation of Sevelamer and Mortality among Hemodialysis Patients Treated with Calcium-Based Phosphate Binders.Clin J Am Soc Nephrol. 2017 Sep 7;12(9):1489-1497. doi: 10.2215/CJN.13091216. Epub 2017 Jul 19. Clin J Am Soc Nephrol. 2017. PMID: 28724618 Free PMC article.
-
Sevelamer Versus Calcium-Based Binders for Treatment of Hyperphosphatemia in CKD: A Meta-Analysis of Randomized Controlled Trials.Clin J Am Soc Nephrol. 2016 Feb 5;11(2):232-44. doi: 10.2215/CJN.06800615. Epub 2015 Dec 14. Clin J Am Soc Nephrol. 2016. PMID: 26668024 Free PMC article. Review.
-
The Phosphate Binder Ferric Citrate and Mineral Metabolism and Inflammatory Markers in Maintenance Dialysis Patients: Results From Prespecified Analyses of a Randomized Clinical Trial.Am J Kidney Dis. 2015 Sep;66(3):479-88. doi: 10.1053/j.ajkd.2015.03.013. Epub 2015 May 7. Am J Kidney Dis. 2015. PMID: 25958079 Free PMC article. Clinical Trial.
References
-
- Ketteler M, Block GA, Evenepoel P, Fukagawa M, Herzog CA, McCann L, et al. Diagnosis, evaluation, prevention, and treatment of chronic kidney disease-mineral and bone disorder: synopsis of the kidney disease: improving global outcomes 2017 clinical practice guideline update. Ann Intern Med. 2018;168(6):422–30. doi: 10.7326/M17-2640. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
