

Multicenter validation of a galactomannan chemiluminescence immunoassay for the diagnosis of pulmonary aspergillosis on serum of patients with hematological disease
- PMID: 39835823
- PMCID: PMC11837514
- DOI: 10.1128/jcm.01053-24
Multicenter validation of a galactomannan chemiluminescence immunoassay for the diagnosis of pulmonary aspergillosis on serum of patients with hematological disease
Erratum in
-
Correction for Lamberink et al., "Multicenter validation of a galactomannan chemiluminescence immunoassay for the diagnosis of pulmonary aspergillosis on serum of patients with hematological disease".J Clin Microbiol. 2025 May 14;63(5):e0039425. doi: 10.1128/jcm.00394-25. Epub 2025 Mar 25. J Clin Microbiol. 2025. PMID: 40130834 Free PMC article. No abstract available.
Abstract
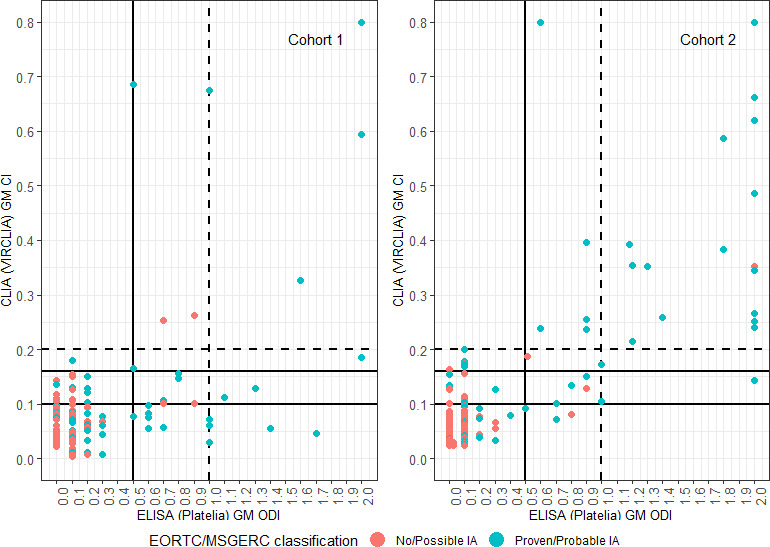
An accurate diagnosis of invasive aspergillosis (IA) in patients with underlying hematological malignancies relies heavily on galactomannan detection. In this study, we compared the VirCLIA chemiluminescence immunoassay (CLIA) with the frequently used Platelia enzyme-linked immunosorbent assay (ELISA) on serum from hematology patients with suspected IA. Patients were categorized according to EORTC/MSGERC 2020 definitions into proven/probable IA and possible/no IA. The first cohort included 161 patients at four centers, and the VirCLIA manufacturer's cutoff of 0.200 was evaluated. Next, the optimal cutoff was determined using the Youden's index. In a second independent cohort of 189 patients from four centers, this optimal cutoff was evaluated again. In the first cohort, sensitivities and specificities for probable/proven IA were 21.1% and 100.0% for ELISA (1.0 cutoff) and 36.6% and 95.6% (0.5 cutoff), compared to 11.3% and 97.8% for CLIA (0.200 cutoff). In the second cohort, the sensitivities of ELISA and CLIA were comparable (ELISA ≥ 1.0: 33.3%, CLIA ≥ 0.200: 38.1%). The area under the ROC curve was lower for CLIA than for ELISA in the first cohort (65.0% vs 78.7%, P = 0.005) but comparable in the second cohort (79.5% vs 81.3%, P = 0.649). Youden's index identified 0.100 as the optimal CLIA cutoff with sensitivities of 35.2% and 61.9% in cohorts 1 and 2, respectively, at slightly reduced specificities of 85.6% and 90.5%. While the sensitivity of both assays was low to moderate at best, in patients with a high pre-test probability, we suggest 0.100 as the cutoff for the VirCLIA assay.IMPORTANCEThis study demonstrates a comparable performance of the novel chemiluminescence immunoassay (CLIA) and the conventionally used enzyme-linked immunosorbent assay for galactomannan serum testing in hematological patients at high risk for invasive aspergillosis. In patients with a high pre-test probability, a lower CLIA cutoff of 0.100 is preferred.
Keywords: chemiluminescence assay; galactomannan; invasive aspergillosis.
Conflict of interest statement
The authors declare a conflict of interest (see Acknowledgments).
Figures
Similar articles
-
Diagnostic accuracy of PCR alone compared to galactomannan in bronchoalveolar lavage fluid for diagnosis of invasive pulmonary aspergillosis: a systematic review.J Clin Microbiol. 2012 Nov;50(11):3652-8. doi: 10.1128/JCM.00942-12. Epub 2012 Sep 5. J Clin Microbiol. 2012. PMID: 22952268 Free PMC article.
-
Evaluation of a novel aspergillus IgG lateral flow assay for the diagnosis of non-neutropenic patients with acute and subacute invasive aspergillosis.Front Cell Infect Microbiol. 2025 Jun 20;15:1599425. doi: 10.3389/fcimb.2025.1599425. eCollection 2025. Front Cell Infect Microbiol. 2025. PMID: 40621162 Free PMC article.
-
Utility of bronchoalveolar lavage fluid galactomannan alone or in combination with PCR for the diagnosis of invasive aspergillosis in adult hematology patients: a systematic review and meta-analysis.Crit Rev Microbiol. 2015 Feb;41(1):124-34. doi: 10.3109/1040841X.2013.804033. Epub 2013 Jun 25. Crit Rev Microbiol. 2015. PMID: 23799871
-
Galactomannan detection for invasive aspergillosis in immunocompromized patients.Cochrane Database Syst Rev. 2008 Oct 8;(4):CD007394. doi: 10.1002/14651858.CD007394. Cochrane Database Syst Rev. 2008. Update in: Cochrane Database Syst Rev. 2015 Dec 30;(12):CD007394. doi: 10.1002/14651858.CD007394.pub2. PMID: 18843747 Updated.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
References
-
- Leeflang MMG, Debets-Ossenkopp YJ, Wang J, Visser CE, Scholten R, Hooft L, Bijlmer HA, Reitsma JB, Zhang M, Bossuyt PMM, Vandenbroucke-Grauls CM. 2015. Galactomannan detection for invasive aspergillosis in immunocompromised patients. Cochrane Database Syst Rev 2015:CD007394. doi:10.1002/14651858.CD007394.pub2 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
