

CA-125 as a Biomarker in Renal Medullary Carcinoma: Integrated Molecular Profiling, Functional Characterization, and Prospective Clinical Validation
- PMID: 39836407
- PMCID: PMC11913570
- DOI: 10.1158/1078-0432.CCR-24-3324
CA-125 as a Biomarker in Renal Medullary Carcinoma: Integrated Molecular Profiling, Functional Characterization, and Prospective Clinical Validation
Abstract
Purpose: Renal medullary carcinoma (RMC) is a highly aggressive malignancy defined by the loss of the SMARCB1 tumor suppressor. It mainly affects young individuals of African descent with sickle cell trait, and it is resistant to conventional therapies used for other renal cell carcinomas. This study aimed to identify potential biomarkers for early detection and disease monitoring of RMC.
Experimental design: Integrated profiling of primary untreated RMC tumor tissues and paired adjacent kidney controls was performed using RNA sequencing and histone chromatin immunoprecipitation sequencing. The expression of serum cancer antigen 125 (CA-125), was prospectively evaluated in 47 patients with RMC. Functional studies were conducted in RMC cell lines to assess the effects of SMARCB1 reexpression.
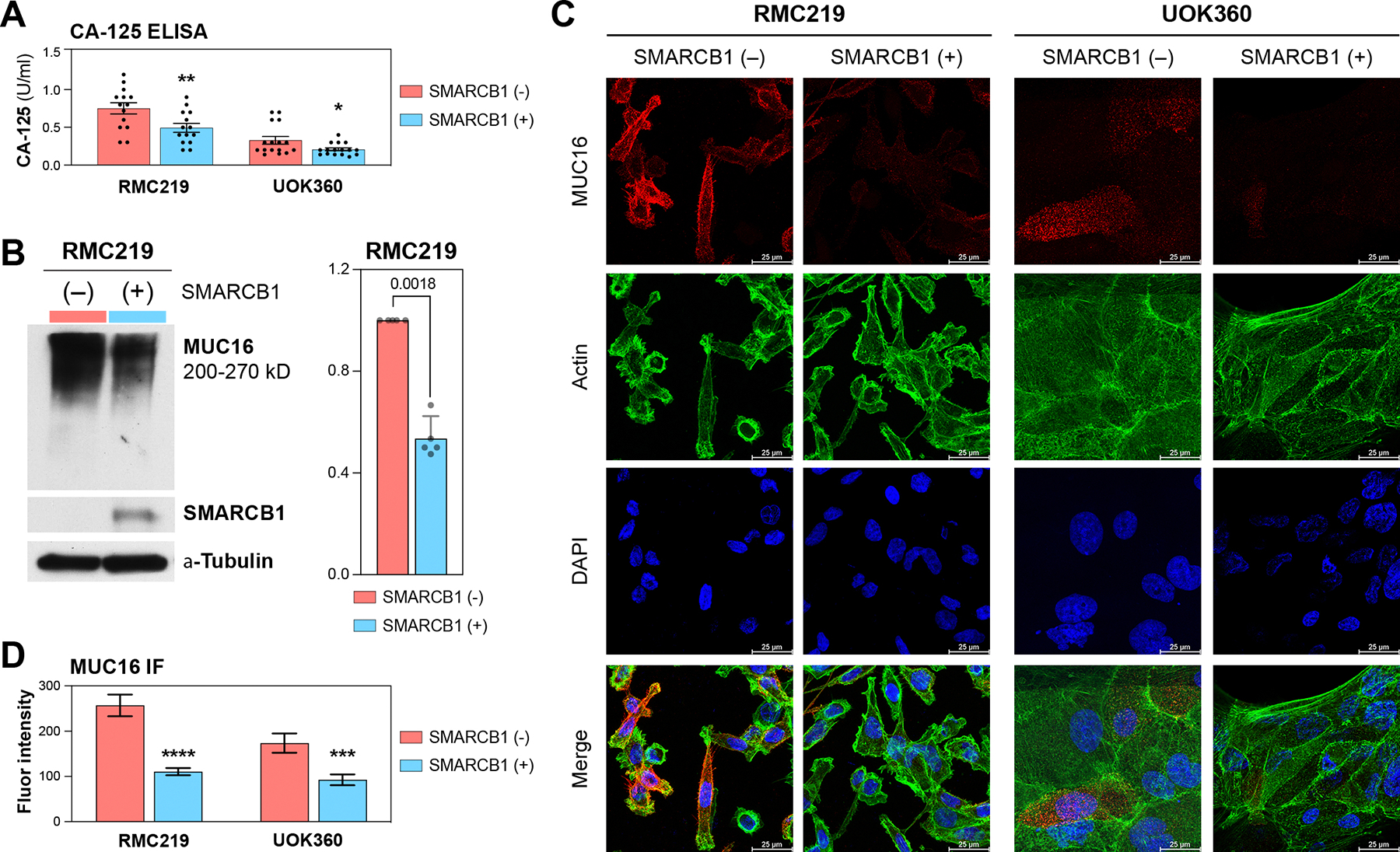
Results: MUC16, encoding for CA-125, was identified as one of the top upregulated genes in RMC tissues, with concomitant enrichment of active histone marks H3K4me3 and H3K27ac at its promoter. Elevated serum CA-125 levels were found in 31 of 47 (66%) patients with RMC and correlated significantly with metastatic tumor burden (P = 0.03). Functional studies in RMC cell lines demonstrated that SMARCB1 reexpression significantly reduced MUC16 expression.
Conclusions: The correlation between serum CA-125 levels and metastatic burden suggests that CA-125 is a clinically relevant biomarker for RMC. These findings support further exploration of CA-125 for disease monitoring and targeted therapeutics in RMC.
©2025 American Association for Cancer Research.
Figures




References
MeSH terms
Substances
Grants and funding
- P30 CA016672/CA/NCI NIH HHS/United States
- RP210227/Cancer Prevention and Research Institute of Texas (CPRIT)
- R35 CA231993/CA/NCI NIH HHS/United States
- Translational Research Award/V Foundation for Cancer Research (VFCR)
- CA125123/National Cancer Institute (NCI)
- Advanced Discovery Award/Kidney Cancer Association (KCA)
- P42 ES027725/ES/NIEHS NIH HHS/United States
- R37CA288448/National Cancer Institute (NCI)
- P30 ES030285/ES/NIEHS NIH HHS/United States
- P30 CA125123/CA/NCI NIH HHS/United States
- S10 OD023469/OD/NIH HHS/United States
- R37 CA288448/CA/NCI NIH HHS/United States
- KC200096P1/U.S. Department of Defense (DOD)
- P30 DK056338/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
