

Clinical Manifestations and Challenges in Adolescent and Adult Females With Classic Congenital Adrenal Hyperplasia Due to 21-Hydroxylase Deficiency
- PMID: 39836618
- PMCID: PMC11749906
- DOI: 10.1210/clinem/dgae696
Clinical Manifestations and Challenges in Adolescent and Adult Females With Classic Congenital Adrenal Hyperplasia Due to 21-Hydroxylase Deficiency
Abstract
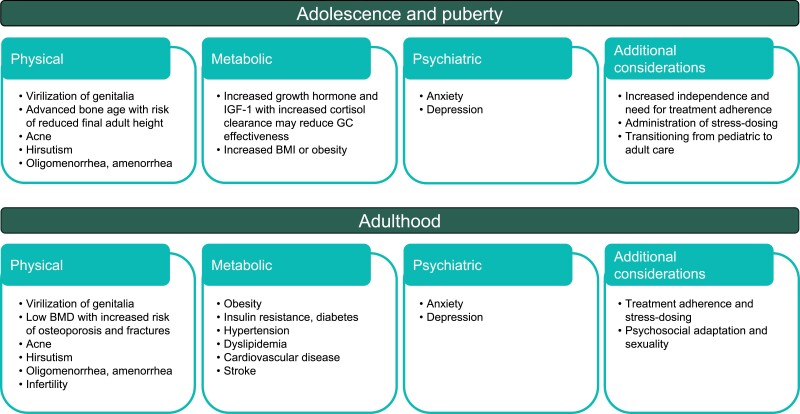
Classic congenital adrenal hyperplasia due to 21-hydroxylase deficiency (CAH) is a rare genetic condition that results in cortisol deficiency and excess production of adrenal androgens. While the introduction of newborn screening for CAH has reduced morbidity and mortality, management of CAH remains challenging. Lifelong treatment with glucocorticoids is required to replace the endogenous cortisol deficiency and reduce excess adrenal androgens. Undertreatment or overtreatment with glucocorticoids can lead to multiple disease- and treatment-related comorbidities, including impaired growth and compromised final height, menstrual irregularities and reduced fertility in females, and long-term cardiometabolic complications. In addition to avoiding adrenal crisis and sudden death, treatment goals in adolescent females with CAH are to obtain normal growth and bone maturation and normal timing of puberty. Management of adolescents is particularly challenging due to changes in growth and sex hormone levels that can lead to inadequate suppression of adrenal androgens and increasing independence that can affect treatment adherence. During the transition to adult care, treatment goals focus on preventing symptoms of hyperandrogenism, preserving menstrual regularity and fertility, and providing education and support for issues related to sexuality, atypical genitalia, and/or complications from previous surgical treatment. In addition, patients must be monitored continuously to prevent long-term complications such as decreased bone mineral density, obesity, diabetes, and hypertension. In this review, we discuss the challenges faced by adolescent and adult females with CAH and provide guidance to health-care professionals to help patients to navigate these challenges.
Keywords: adolescence; congenital adrenal hyperplasia; females; long-term complications; treatment.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- Kamrath C, Wettstaedt L, Boettcher C, Hartmann MF, Wudy SA. Androgen excess is due to elevated 11-oxygenated androgens in treated children with congenital adrenal hyperplasia. J Steroid Biochem Mol Biol. 2018;178:221‐228. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
