

Barriers to the Management of Classic Congenital Adrenal Hyperplasia Due to 21-Hydroxylase Deficiency
- PMID: 39836619
- PMCID: PMC11749880
- DOI: 10.1210/clinem/dgae710
Barriers to the Management of Classic Congenital Adrenal Hyperplasia Due to 21-Hydroxylase Deficiency
Abstract
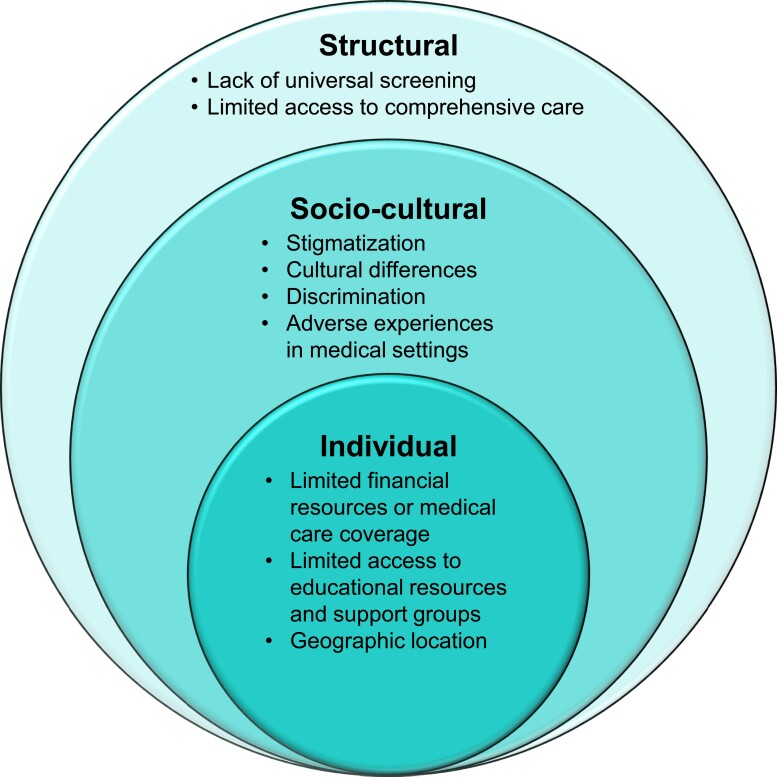
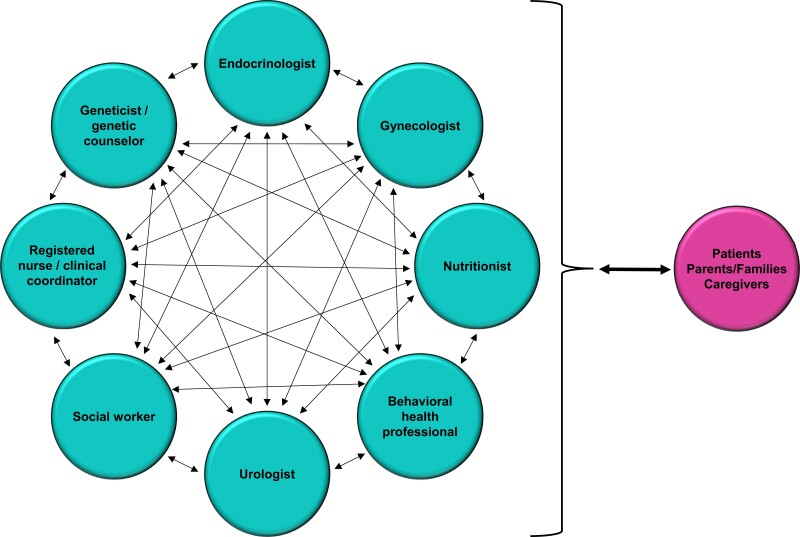
Classic congenital adrenal hyperplasia (CAH) due to 21-hydroxylase deficiency is a rare genetic condition that requires lifelong management from birth. Individuals with CAH and their families often face structural barriers to obtaining comprehensive care and treatment, including limited access to appropriate newborn screening, comprehensive care centers, and medications. Social and cultural barriers to care may include stigmatization, discrimination, and adverse medical experiences. At the individual and family level, comprehensive care may be affected by education, finances, health-care coverage, geographic location, and lack of social supports. These barriers are often further magnified for individuals living in underresourced countries. Inadequate access to comprehensive care and medications increases the risk of life-threatening adrenal crisis and disease-related comorbidities. This review article examines the current structural, sociocultural, and individual barriers that individuals with CAH and their families may face when managing their condition throughout their lifetime.
Keywords: access; barrier; congenital adrenal hyperplasia; education; screening; stigma.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
