

Challenges in Adolescent and Adult Males With Classic Congenital Adrenal Hyperplasia Due to 21-Hydroxylase Deficiency
- PMID: 39836620
- PMCID: PMC11749911
- DOI: 10.1210/clinem/dgae718
Challenges in Adolescent and Adult Males With Classic Congenital Adrenal Hyperplasia Due to 21-Hydroxylase Deficiency
Abstract
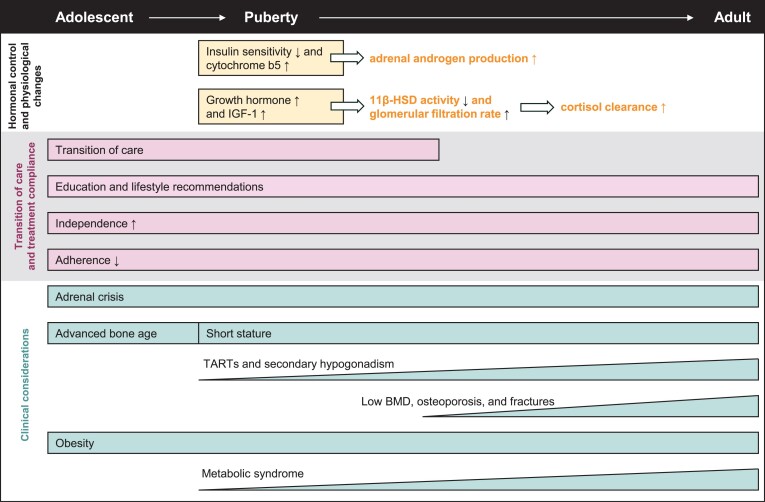
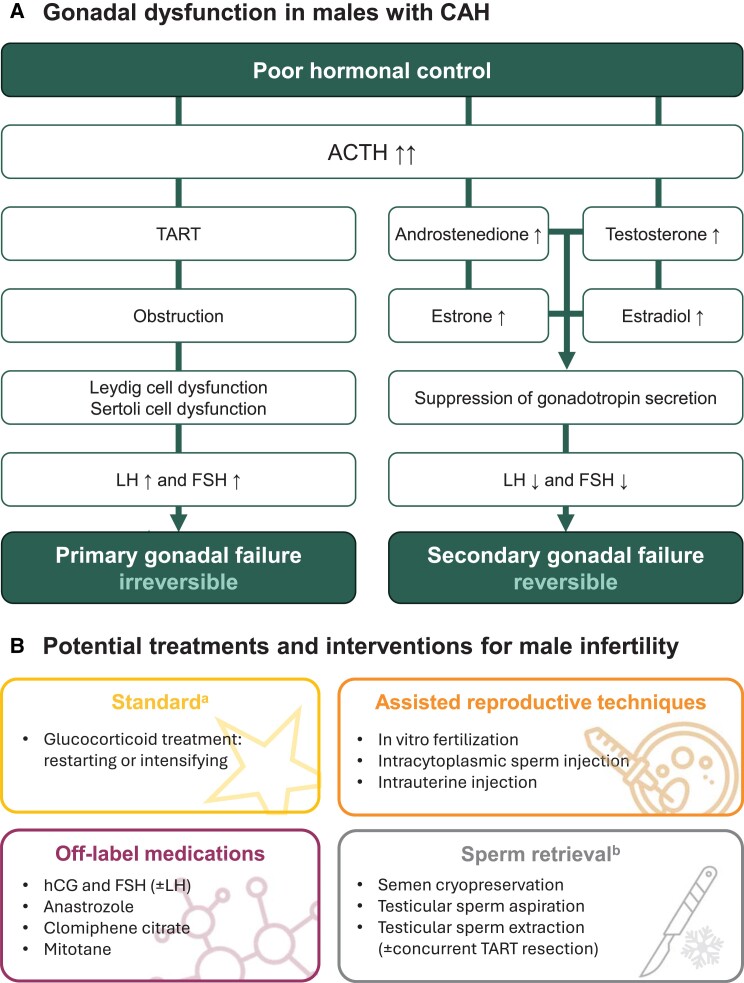
Classic congenital adrenal hyperplasia (CAH) due to 21-hydroxylase deficiency results in severe cortisol and aldosterone deficiency, leading to persistent adrenal stimulation and excess production of ACTH and adrenal androgens. This review examines the clinical considerations and challenges of balancing under- and overtreatment with glucocorticoids in adolescent and adult male individuals with CAH. Adolescents face many unique challenges that can hinder adherence, hormonal control, and transition to independence. Thus, patient education is critical during adolescence, especially in poorly controlled postpubertal males who lack obvious symptoms and may not recognize the long-term consequences of nonadherence, such as reduced final height, reduced reproductive health, poor bone health, obesity, and hypertension. The risk of subfertility/infertility begins early, especially in males with poor hormonal control, who often have reduced sperm counts, small testes, and benign tumors called testicular adrenal rest tumors (TARTs). Even males with good hormonal control can experience subfertility/infertility due to TARTs. In addition, several factors such as hypogonadism and long-term glucocorticoid treatment can predispose males with CAH to poor bone health (eg, low bone mineral density, increased risk of osteoporosis/osteopenia and fractures) and metabolic syndrome (eg, obesity, insulin resistance, dyslipidemia, and hypertension). Regular monitoring is recommended, with glucocorticoid dose optimization and prophylactic treatment to maximize future fertility potential and protect long-term bone health. Early implementation of lifestyle interventions and medical treatment are needed to address cardiometabolic consequences.
Keywords: bone health; cardiometabolic health; congenital adrenal hyperplasia; hypergonadotropic hypogonadism; testicular adrenal rest tumors; transition of care.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
Similar articles
-
Clinical Manifestations and Challenges in Adolescent and Adult Females With Classic Congenital Adrenal Hyperplasia Due to 21-Hydroxylase Deficiency.J Clin Endocrinol Metab. 2025 Jan 21;110(Supplement_1):S37-S45. doi: 10.1210/clinem/dgae696. J Clin Endocrinol Metab. 2025. PMID: 39836618 Free PMC article. Review.
-
Glucocorticoid replacement regimens for treating congenital adrenal hyperplasia.Cochrane Database Syst Rev. 2020 Mar 19;3(3):CD012517. doi: 10.1002/14651858.CD012517.pub2. Cochrane Database Syst Rev. 2020. PMID: 32190901 Free PMC article.
-
High prevalence of reduced fecundity in men with congenital adrenal hyperplasia.J Clin Endocrinol Metab. 2009 May;94(5):1665-70. doi: 10.1210/jc.2008-1414. Epub 2009 Mar 3. J Clin Endocrinol Metab. 2009. PMID: 19258407
-
Testicular adrenal rest tumors in congenital adrenal hyperplasia-cross-sectional study of 51 Croatian male patients.Eur J Pediatr. 2017 Oct;176(10):1393-1404. doi: 10.1007/s00431-017-3008-7. Epub 2017 Sep 6. Eur J Pediatr. 2017. PMID: 28879515
-
Restoration of reproductive capacity in a male patient with congenital adrenal hyperplasia and bilateral testicular adrenal rest tumors (TARTs) after six months of glucocorticoid intensification: A case report.Medicine (Baltimore). 2023 Dec 8;102(49):e36061. doi: 10.1097/MD.0000000000036061. Medicine (Baltimore). 2023. PMID: 38065885 Free PMC article.
Cited by
-
Global clinical trials on stem cell therapy for autoimmune diseases: trends and future directions.Front Immunol. 2025 Jul 24;16:1616231. doi: 10.3389/fimmu.2025.1616231. eCollection 2025. Front Immunol. 2025. PMID: 40777013 Free PMC article.
References
-
- Merke DP, Auchus RJ. Congenital adrenal hyperplasia due to 21-hydroxylase deficiency. N Engl J Med. 2020;383(13):1248‐1261. - PubMed
-
- van der Straaten S, Springer A, Zecic A, et al. The External Genitalia Score (EGS): a European multicenter validation study. J Clin Endocrinol Metab. 2020;105(3):e222‐e230. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
