

Clinical Manifestations and Treatment Challenges in Infants and Children With Classic Congenital Adrenal Hyperplasia Due to 21-Hydroxylase Deficiency
- PMID: 39836622
- PMCID: PMC11749889
- DOI: 10.1210/clinem/dgae563
Clinical Manifestations and Treatment Challenges in Infants and Children With Classic Congenital Adrenal Hyperplasia Due to 21-Hydroxylase Deficiency
Abstract
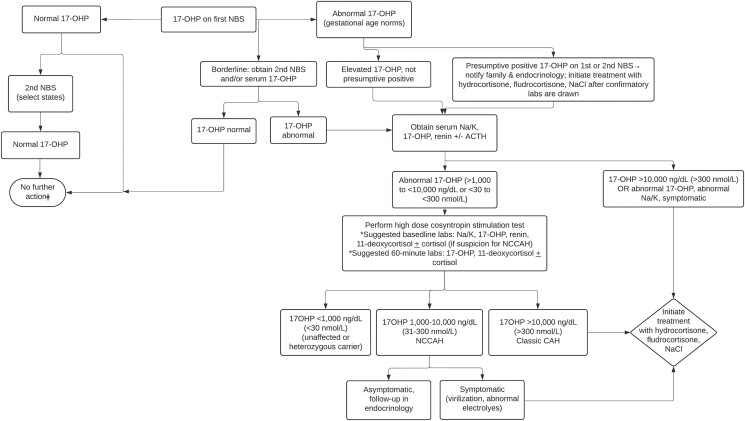
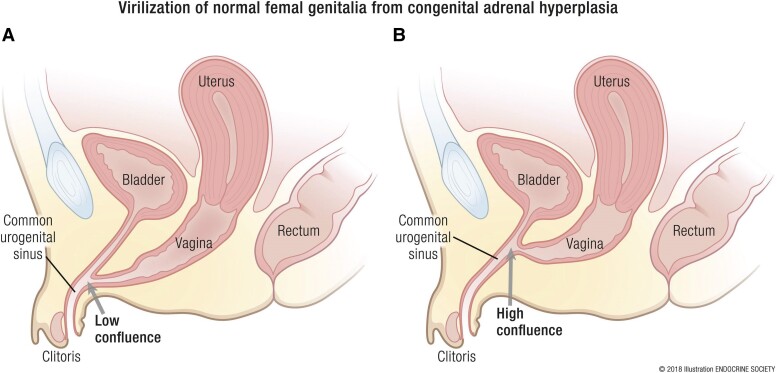
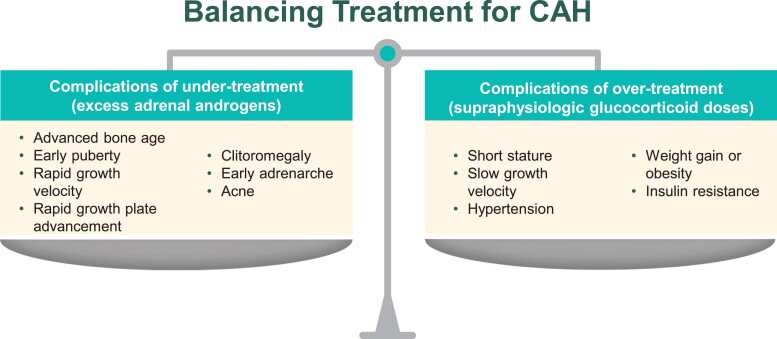
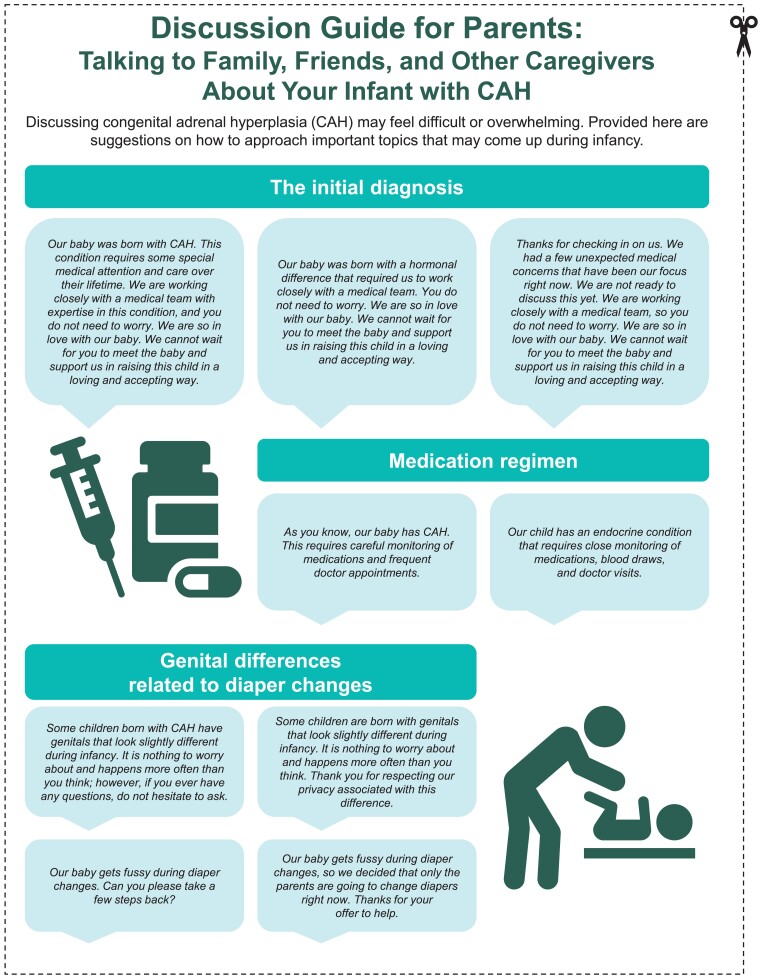
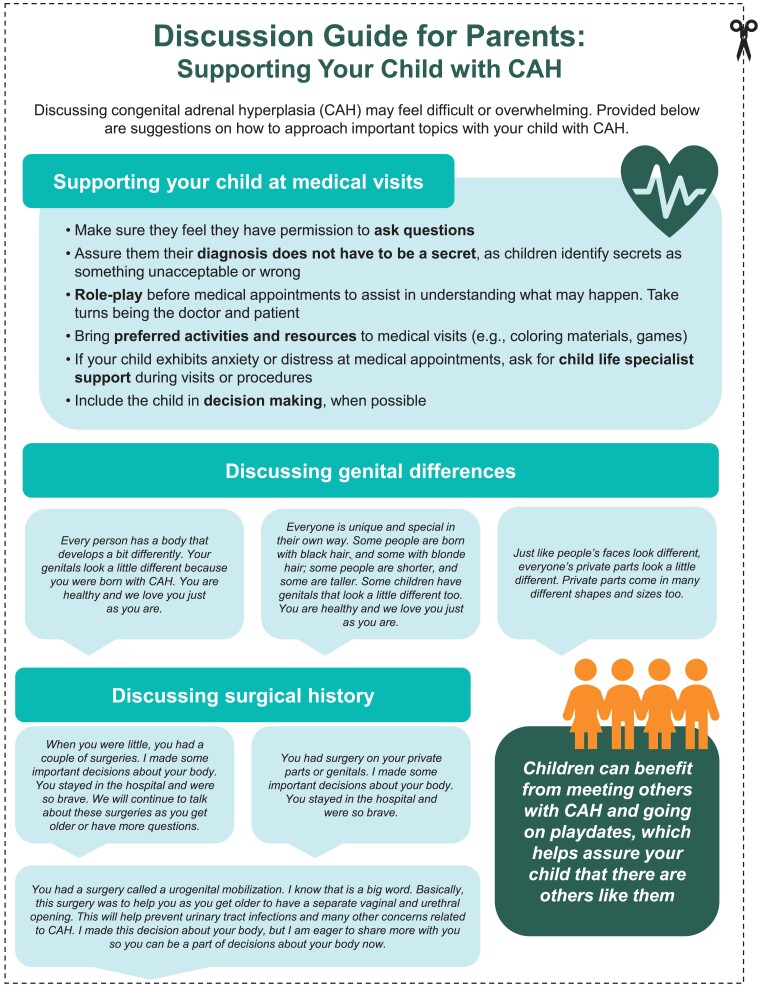
The most common form of congenital adrenal hyperplasia (CAH) is secondary to 21-hydroxylase deficiency (21OHD). This review will summarize the clinical manifestations, recommended treatments, monitoring, clinical challenges and management strategy, and treatment challenges in special situations for infants and children with classic CAH due to 21OHD. Specifically, we review newborn screening and the initial diagnosis, glucocorticoid and mineralocorticoid treatment, and recommended monitoring, including anthropometric and laboratory measures. Children with CAH may have premature adrenarche, precocious puberty, and early growth plate closure and have an increased risk of hypertension and overweight/obesity. Many 46,XX individuals will also have genital differences, which may include clitoromegaly and/or a urogenital sinus. We review psychosocial and surgical considerations, including suggestions on how to talk with children, family, and caregivers about bodily difference. These suggestions may be used by families and/or providers caring for individuals with CAH.
Keywords: 17-hydroxyprogesterone; 21-hydroxylase deficiency; congenital adrenal hyperplasia; fludrocortisone; hydrocortisone.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- Pang S, Spence DA, New MI. Newborn screening for congenital adrenal hyperplasia with special reference to screening in Alaska. Ann N Y Acad Sci. 1985;458:90‐102. - PubMed
-
- Conlon TA, Hawkes CP, Brady J, Loeber JG, Murphy N. International newborn screening practices for the early detection of congenital adrenal hyperplasia. Horm Res Paediatr. 2024;97(2):113‐125. - PubMed
-
- Sarafoglou K, Banks K, Gaviglio A, Hietala A, McCann M, Thomas W. Comparison of one-tier and two-tier newborn screening metrics for congenital adrenal hyperplasia. Pediatrics. 2012;130(5):e1261‐e1268. - PubMed
-
- Chan CL, McFann K, Taylor L, Wright D, Zeitler PS, Barker JM. Congenital adrenal hyperplasia and the second newborn screen. J Pediatr. 2013;163(1):109‐113.e1. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
