

Pembrolizumab and chemotherapy in high-risk, early-stage, ER+/HER2- breast cancer: a randomized phase 3 trial
- PMID: 39838117
- PMCID: PMC11835712
- DOI: 10.1038/s41591-024-03415-7
Pembrolizumab and chemotherapy in high-risk, early-stage, ER+/HER2- breast cancer: a randomized phase 3 trial
Abstract
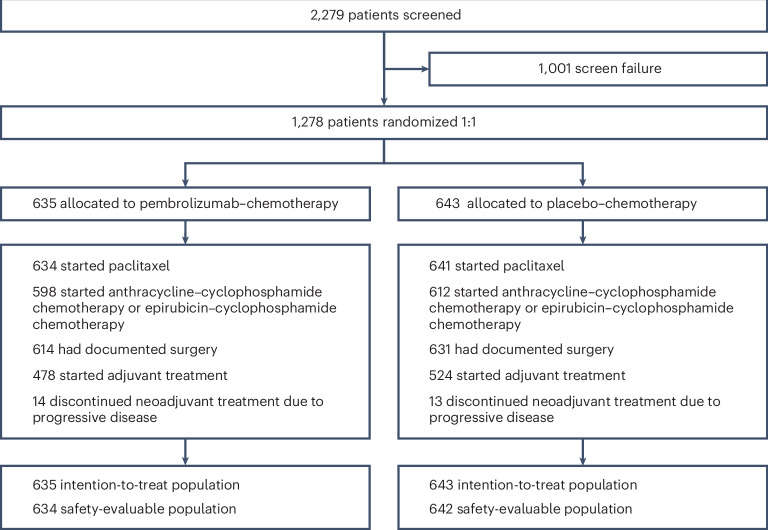
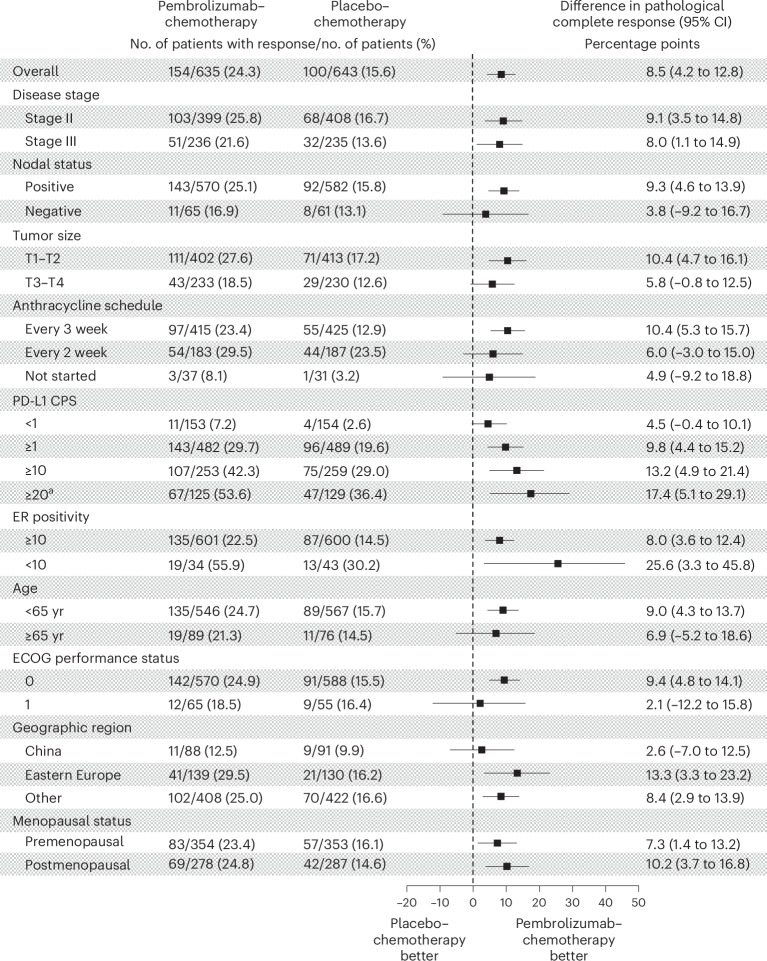
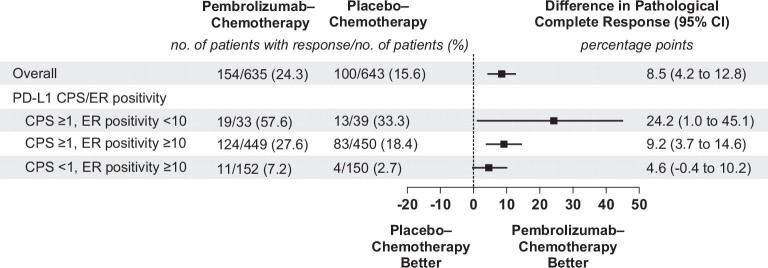
Addition of pembrolizumab to neoadjuvant chemotherapy followed by adjuvant pembrolizumab improved outcomes in patients with high-risk, early-stage, triple-negative breast cancer. However, whether the addition of neoadjuvant pembrolizumab to chemotherapy would improve outcomes in high-risk, early-stage, estrogen receptor-positive/human epidermal growth factor receptor 2-negative (ER+/HER2-) breast cancer remains unclear. We conducted a double-blind, placebo-controlled phase 3 study (KEYNOTE-756) in which patients with previously untreated ER+/HER2- grade 3 high-risk invasive breast cancer (T1c-2 (≥2 cm), cN1-2 or T3-4, cN0-2) were randomly assigned (1:1) to neoadjuvant pembrolizumab 200 mg or placebo Q3W given with paclitaxel QW for 12 weeks, followed by four cycles of doxorubicin or epirubicin plus cyclophosphamide Q2W or Q3W. After surgery (with/without adjuvant radiation therapy), patients received adjuvant pembrolizumab or placebo for nine cycles plus adjuvant endocrine therapy. Dual primary endpoints were pathological complete response and event-free survival in the intention-to-treat population. In total, 635 patients were assigned to the pembrolizumab-chemotherapy arm and 643 to the placebo-chemotherapy arm. At the study's prespecified first interim analysis, the pathological complete response rate was 24.3% (95% confidence interval (CI), 21.0-27.8%) in the pembrolizumab-chemotherapy arm and 15.6% (95% CI, 12.8-18.6%) in the placebo-chemotherapy arm (estimated treatment difference, 8.5 percentage points; 95% CI, 4.2-12.8; P = 0.00005). Event-free survival was not mature in this analysis. During the neoadjuvant phase, treatment-related adverse events of grade ≥3 were reported in 52.5% and 46.4% of patients in the pembrolizumab-chemotherapy and placebo-chemotherapy arms, respectively. In summary, the addition of pembrolizumab to neoadjuvant chemotherapy significantly improved the pathological complete response rate in patients with high-risk, early-stage ER+/HER2- breast cancer. Safety was consistent with the known profiles of each study treatment. Follow-up continues for event-free survival. ClinicalTrials.gov identifier: NCT03725059 .
© 2025. Merck & Co., Inc., Rahway, NJ, USA and its affiliates, and the Author(s).
Conflict of interest statement
Competing interests: F.C. receives consultancy honorarium from Amgen, Astellas/Medivation, AstraZeneca, Celgene, Daiichi Sankyo, Eisai, GE Oncology, Genentech, Gilead, GlaxoSmithKline, Iqvia, Macrogenics, Medscape, Merck Sharp & Dohme, Merus BV, Mylan, Mundipharma, Novartis, Pfizer, Pierre Fabre, prIME Oncology, Roche, Sanofi, Samsung, Bioepis, Seagen, Teva, and Touchime. J.O’.S. receives honoraria for consulting and/or advisory boards from AbbVie, Agendia, Amgen, Aptitude Health, AstraZeneca, BioNTech, Byondis, Carrick Therapeutics, Daiichi Sankyo Company, DAVA Oncology, Eisai, Eli Lilly, Fishawack Health, G1 Therapeutics, Genzyme, GlaxoSmithKline, Genentech, Gilead, Loxo Oncology, Merck Sharp & Dohme, Novartis, Ontada, Pfizer, Pierre Fabre Pharmaceuticals, Puma Biotechnology, Roche, Samsung Bioepis, Sanofi, Seagen, Stemline Therapeutics, Taiho Oncology and Veru. H.M. receives consultancy fees from Amgen, AstraZeneca, Bristol Myers Squibb, Calithera, Celgene, Crown Bioscience, Daiichi Sankyo, Eli Lilly, Genentech/Roche, Gilead, Immunomedics, Merck Sharp & Dohme, OBI Pharma, Peregrine, Pfizer, Puma, Seattle Genetics, Spectrum Pharmaceuticals, Syndax Pharmaceuticals and TapImmune and research support from Bristol Myers Squibb, BTG, MedImmune/AstraZeneca and Merck Sharp & DohmeD. P.S. receives consultant fees from or received honoraria from AstraZeneca, Bayer, Boehringer Ingelheim, Merck, Novartis, Pfizer, Puma, Roche, Eisai and Celgene; and receives grant funding (to institution) from Astellas, AstraZeneca, Genentech, Novartis, Oncogenex, Roche and Medivation. J.C. is a consultant/advisor for Roche, AstraZeneca, Seattle Genetics, Daiichi Sankyo, Lilly, Merck Sharp & Dohme, Leuko, Bioasis, Clovis Oncology, Boehringer Ingelheim, Ellipses, Hibercell, BioInvent, Gemoab, Gilead, Menarini, Zymeworks, Reveal Genomics, Scorpion Therapeutics, Expres2ion Biotechnologies, Jazz Pharmaceuticals, Abbvie, BridgeBio, Biontech and Biocon; receives honoraria from Roche, Novartis, Eisai, Pfizer, Lilly, Merck Sharp & Dohme, Daiichi Sankyo, AstraZeneca, Gilead and Stemline Therapeutics; receives research funding (to institution) from Roche, Ariad Pharmaceuticals, AstraZeneca, Baxalta GMBH/Servier Affaires, Bayer Healthcare, Eisai, F. Hoffman-La Roche, Guardant Health, Merck Sharp & Dohme, Pfizer, Piqur Therapeutics, Iqvia and Queen Mary University of London; holds stock in MAJ3 Capital, Leuko (relative); has receives travel, accommodation and expenses from Roche, Novartis, Eisai, Pfizer, Daiichi Sankyo, AstraZeneca, Gilead, Merck Sharp & Dohme and Stemline Therapeutics; listed on patents for pharmaceutical combinations of a Pi3k inhibitor and a microtubule destabilizing agent (J.C. Castán, A.P. Giménez, V.S. Elizalde; WO 2014/199294 A; ISSUED) and for Her2 as a predictor of response to dual HER2 blockade in the absence of cytotoxic therapy (A. Prat, A. Llombart, J.C.; US 2019/0338368 A1; LICENSED). N.H. is a consultant for Gilead, Hoffmann-La Roche and Seagen; holds business ownership in the West German Study Group; and receives honoraria for lectures from AstraZeneca, Daiichi Sankyo, F. Gilead, Hoffmann-La Roche, Merck Sharp & Dohme, Lilly, Novartis, Pfizer Pharma GmbH, Pierre Fabre Pharmaceuticals, Seagen, Viatris and Zuelligpharma. M.L.T. is a consultant for AstraZeneca, Blueprint Medicines, Daiichi Sankyo, Genentech, Gilead (DSMC), GlaxoSmithKline, G1 Therapeutics (DSMC), Guardant, Menarini Stemline, Merck, Natera, Novartis, Pfizer, RefleXion, Replicate and Sanofi Aventis; receives grant/research support (institutional) from Arvinas, AstraZeneca, Bayer, Genentech/Roche, GlaxoSmithKline, Hummingbird Biosciences, Merck, OncoSec Medical and Pfizer. D.W.C. is a consultant/advisor for AstraZeneca, Exact Sciences, Eisai, Gilead, GlaxoSmithKline, Inflex, Inivata/Neogenomics, Lilly, Merck Sharp & Dohme, Novartis, Pfizer, Roche and SAGA; receives research support to institutions from AstraZeneca, GlaxoSmithKline, Inivata, Knight, Merck Sharp & Dohme, Pfizer and Roche; is a member of a trial steering committee for AstraZeneca, Merck Sharp & Dohme and GlaxoSmithKline; holds a patent (US62/675,228) for methods of treating cancers characterized by a high expression level of spindle and kinetochore-associated complex subunit 3 (ska3) gene. P.A.F. receives consulting fees from Agendia, AstraZeneca, Daiichi Sankyo, Eisai, Hexal, Lilly, Merck Sharp & Dohme, a subsidiary of Merck & Co., Novartis, Pfizer, Pierre Fabre, Roche and Seagen; receives fees for non-CME services received directly from commercial interests or their agents (Daiichi Sankyo, Lilly, Novartis and Seagen); and receives research grants from Biontech and Cepheid. D.L. is a consultant/advisor for AstraZeneca and Merck Sharp & Dohme and receives honoraria from Novartis, Pfizer, Roche, Lilly, Gilead, Merck Sharp & Dohme and AstraZeneca. Y.H.P. receives consultancy or advisory fees from AstraZeneca, Eisai, Eli Lilly Export S.A. Puerto Rico Branch, Novartis, Pfizer and Roche; and receives research funding from AstraZeneca, Merck Sharp & Dohme, Novartis, Pfizer and Roche. G.R. receives honoraria from AstraZeneca, Gilead, Med-Gen Sol, Merck Sharp & Dohme, Roche, Novartis, Lilly, Swixx and Pfizer. L.S. is a consultant/advisor for Novartis, Daiichi Pharma, AstraZeneca, Eli Lilly, Precede and Seagen; and received institutional research support from Merck, Genentech, Gilead and Eli Lilly. S.-A.I. is a consultant/advisor for AstraZeneca, Novartis, Roche/Genentech, Pfizer, Amgen, Hanmi, Lilly, GlaxoSmithKline, Merck Sharp & Dohme, Daiichi Sankyo, Idience and Bertis; receives research funding to institutions from AstraZeneca, Pfizer, Roche/Genentech, Daewoong Pharmaceutical, Eisai Korea and Boryung Pharm. R.H. is a consultant/advisor for Amgen, AstraZeneca, Bristol Myers Squibb, Eisai, Eli Lilly and Company, Janssen, Merck KGaA, Merck Sharp & Dohme, Novartis, OncoSec Medical Incorporated, Pfizer Australia, Roche Products Pty, Seagen, Takeda and Zai Lab; receives honorarium from AstraZeneca, Eli Lilly, Janssen, Merck Sharp & Dohme and Novartis; and receives research funding (to institutions) from AstraZeneca, BMS, Corvus, Eisai, Eli Lilly, Janssen, Merck Sharp & Dohme, Novartis, Oncosec, Roche and Seagen. T.T. receives honoraria from Daiichi Sankyo, Chugai and Eli Lilly. F.A. receives research grants (to institutions) from AstraZeneca, Daiichi Sankyo, Lilly, Novartis, Pfizer and Roche. Y.D., L.J., V.K. and K.T. are employees of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA, and stockholders in Merck & Co., Inc. A.B. is a consultant/advisor for Pfizer, Novartis, Genentech, Merck & Co., Radius Health, Immunomedics/Gilead, Sanofi, Daiichi Pharma/AstraZeneca, Phillips, Eli Lilly and Foundation Medicine and research/grant (to institution) from Genentech, Novartis, Pfizer, Merck & Co., Sanofi, Radius Health, Immunomedics/Gilead, Daiichi Pharma/AstraZeneca and Eli Lilly.
Figures

References
-
- Torrisi, R. et al. Neoadjuvant chemotherapy in hormone receptor-positive/HER2-negative early breast cancer: when, why and what? Crit. Rev. Oncol. Hematol.160, 103280 (2021). - PubMed
-
- Cortazar, P. et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet384, 164–172 (2014). - PubMed
-
- U.S. Department of Health and Human Services, FDA, Oncology Center of Excellence, CDER & CBER. Pathological complete response in neoadjuvant treatment of high-risk early-stage breast cancer: use as an endpoint to support accelerated approval guidance for industry. www.fda.gov/media/83507/download (accessed 21 December 2023).
-
- European Medicines Agency. The role of pathological complete response as an endpoint in neoadjuvant breast cancer studies. www.ema.europa.eu/en/documents/scientific-guideline/draft-guideline-role... (accessed 21 December 2023).
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
