

Neoadjuvant nivolumab and chemotherapy in early estrogen receptor-positive breast cancer: a randomized phase 3 trial
- PMID: 39838118
- PMCID: PMC11835735
- DOI: 10.1038/s41591-024-03414-8
Neoadjuvant nivolumab and chemotherapy in early estrogen receptor-positive breast cancer: a randomized phase 3 trial
Abstract
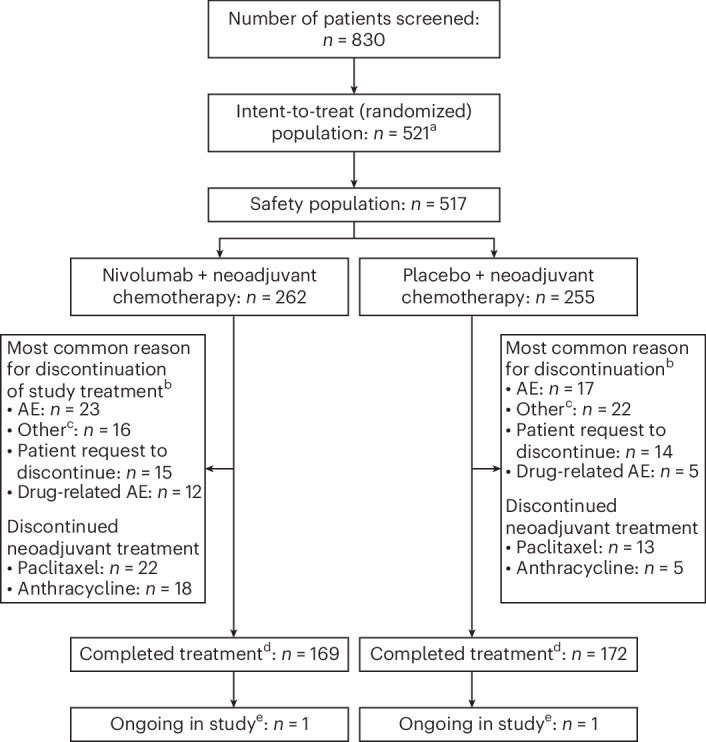
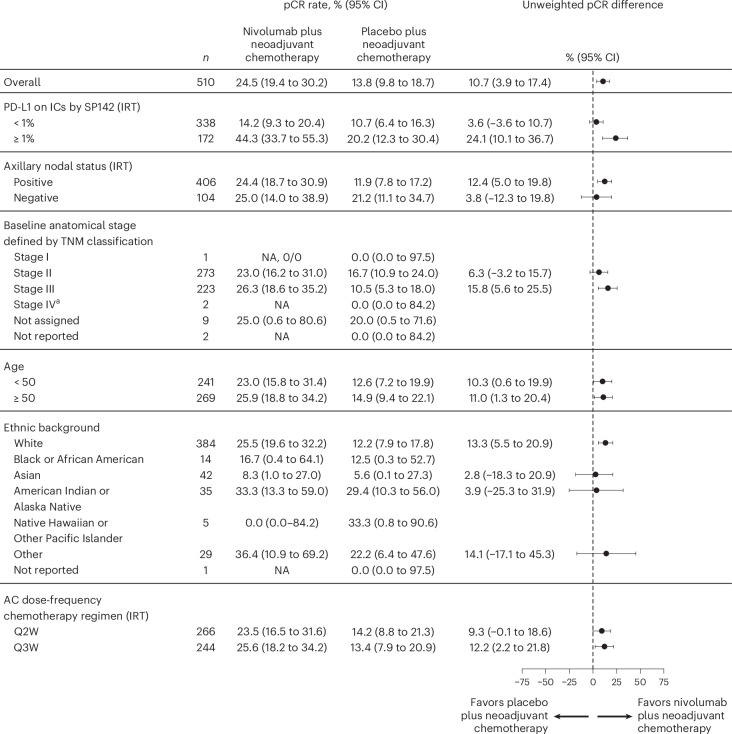
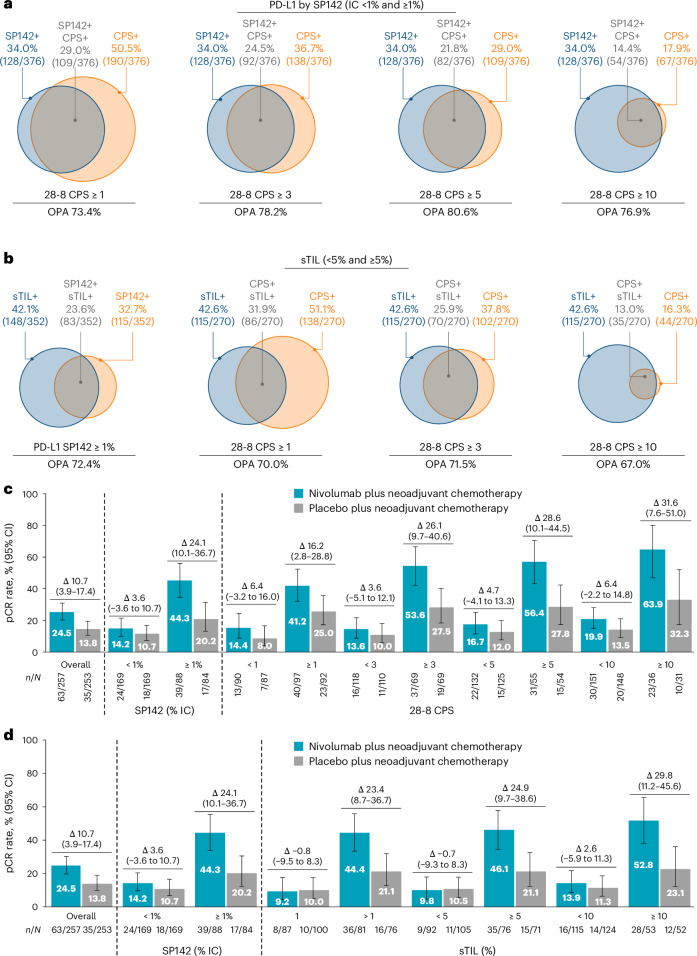
Patients with estrogen receptor-positive (ER+), human epidermal growth factor receptor 2-negative (HER2-) primary breast cancer (BC) have low pathological complete response (pCR) rates with neoadjuvant chemotherapy. A subset of ER+/HER2- BC contains dense lymphocytic infiltration. We hypothesized that addition of an anti-programmed death 1 agent may increase pCR rates in this BC subtype. We conducted a randomized, multicenter, double-blind phase 3 trial to investigate the benefit of adding nivolumab to neoadjuvant chemotherapy in patients with newly diagnosed, high-risk, grade 3 or 2 (ER 1 to ≤10%) ER+/HER2- primary BC. In total, 510 patients were randomized to receive anthracycline and taxane-based chemotherapy with either intravenous nivolumab or placebo. The primary endpoint of pCR was significantly higher in the nivolumab arm compared with placebo (24.5% versus 13.8%; P = 0.0021), with greater benefit observed in patients with programmed death ligand 1-positive tumors (VENTANA SP142 ≥1%: 44.3% versus 20.2% respectively). There were no new safety signals identified. Of the five deaths that occurred in the nivolumab arm, two were related to study drug toxicity; no deaths occurred in the placebo arm. Adding nivolumab to neoadjuvant chemotherapy significantly increased pCR rates in high-risk, early-stage ER+/HER2- BC, particularly among patients with higher stromal tumor-infiltrating lymphocyte levels or programmed death ligand 1 expression, suggesting a new treatment paradigm that emphasizes the role of immunotherapy and T cell immunosurveillance in luminal disease. Clinical trials.gov identifier: NCT04109066.
© 2025. Crown.
Conflict of interest statement
Competing interests: S.L. reports institutional research funding from AstraZeneca/Daiichi Sankyo, Bristol Myers Squibb, Novartis, Puma Biotechnology, Roche-Genentech and Seattle Genetics; consulting fees from Amaroq Therapeutics, Astra Zeneca/Daiichi Sankyo, Bristol Myers Squibb, Domain Therapeutics Gilead, Lilly, Mersana Therapeutics, MSD, Roche-Genentech and Novartis; honoraria from Amaroq Therapeutics, AstraZeneca/Daiichi Sankyo, BioNTech, Bristol Myers Squibb, Domain Therapeutics, Gilead Sciences, Lilly, Mersana Therapeutics, MSD, Novartis and Roche-Genentech; meeting/ travel support from Bristol Myers Squibb and Lilly. R.S. reports consulting fees from Owkin; honoraria from AstraZeneca, Daiichi Sankyo and Exact Sciences; meeting/travel support from AstraZeneca and Daichii Sankyo; leadership position at The International Immuno-Oncology Biomarker Working Group; research support from Bristol Myers Squibb and providing unpaid advice to Case 45. G.C. reports participation on advisory boards for AstraZeneca, Bristol Myers Squibb, Daichii Sankyo, Celcuity, Ellipsis, Exact Science, Gilead, Lilly, Menarini, Merck, Novartis, Pfizer, Roche, Sanofi and Veracyte. S.D. reports institutional research funding from Amgen, AstraZeneca, Bristol Myers Squibb, European Commission, the French government, Lilly, Novartis, Orion, Pierre Fabre, Pfizer, Roche-Genentech, Sanofi and Taiho; meeting/travel support from Novartis, Roche and Seagen; participation on advisory boards for AstraZeneca, Besins, Decibio, Elsan, Gilead and Sanofi; participation on independent data monitoring committee activity for Breast International Group and Pfizer. C.I.R.G. reports honoraria from AstraZeneca, Bristol Myers Squibb, Knight, MSD, Pfizer, Roche and Tecnofarma; participation on data safety monitoring/advisory boards for Bristol Myers Squibb, Pfizer and Sanofi. M.K. reports institutional research funding from AstraZeneca, Bristol Myers Squibb and Roche; honoraria from Bristol Myers Squibb and Gilead; participation on advisory boards for AstraZeneca, BioNTech, Bristol Myers Squibb, MSD and Roche. C.S. reports research funding from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Byondis BV, Daiichi Sankyo, Eisai, Genentech, Gilead, Glaxo, Menarini, Merus, MSD, Novartis, Pfizer, Philips Healthcare, Piere Fabre, Puma Biotechnology, Roche, Sanofi Aventis, Seagen, Synthon and Zymeworks; consulting fees from AstraZeneca, Daiichi Sankyo, Eisai, Gilead, Lilly, MediTech, Novartis, Pfizer, Philips Healthcare, Pharmalex, Piere Fabre, Puma Biotechnology, Roche, Seagen, Synthon and Zymeworks; honoraria from AstraZeneca, Daiichi Sankyo, Exeter Pharmaceuticals, Lilly, Pfizer, Pierre Fabre, Puma Biotechnology and Seagen; payment for expert testimony from AX’s Consulting SARL, Boehringer Ingelheim, Bristol Myers Squibb, Genentech, Innoup, MSD España, Novartis and Sanofi; meeting/travel support from AstraZeneca, Daiichi Sankyo, Eisai Europe, Gilead, Lilly, Novartis, Pfizer, Pierre Fabre, Puma Biotechnology, Roche and Seagen; participation on data safety monitoring/advisory boards for AstraZeneca, Daiichi Sankyo, Eisai Europe, Gilead, Lilly, Menarini, MSD, Novartis, Pfizer, Philips, Pierre Fabre, Roche and Seagen. N.H. reports consulting fees from Daiichi Sankyo, Gilead, Novartis, Pfizer, Roche, Seagen and Viatris; honoraria from AstraZeneca, Daiichi Sankyo, Gilead, Lilly, MSD, Novartis, Pierre Fabre, Pfizer, Roche, Seagen, Viatris and Zuelligpharma; participation on data safety monitoring/advisory boards for Gilead, Roche and Seagen; leadership position at the West German Study Group. E.A.M. reports research funding from Genentech, Gilead and Roche; consulting fees from AstraZeneca, BioNTech, Moderna and MSD; honoraria from MSD; meeting/travel support from MSD; leadership positions at the American Society of Clinical Oncology Board of Directors 2019–2023 and Scientific Advisor for Susan G. Komen. D.A.Y. reports institutional research funding from AbbVie, Ambrx, AstraZeneca, Dana Farber Cancer Institute, Lilly, Roche-Genentech, G1 Therapeutics, Gilead, Incyte, Innocrin Pharmaceuticals, Merck, Novartis, Polyphor, Stemline Therapeutics, US Oncology and UT Southwestern; and consulting fees paid to institution from AstraZeneca, Daiichi Sankyo, Gilead, Integra Connect, Novartis and Stemline Therapeutics. V.G. reports honoraria from AstraZeneca, Daiichi Sankyo, Exact Sciences, Gilead, GlaxoSmithKline, Lilly, Menarini Stemline, Novartis, Roche, and Zentiva; payment for expert testimony from Lilly; meeting/travel support from AstraZeneca and Gilead; institutional patent for Her2DX; and participation on data safety monitoring/advisory boards for AstraZeneca, Daiichi Sankyo, Exact Sciences, Gilead, Lilly, MSD, Novartis, Olema Oncology, Pierre Fabre, Pfizer-Seagen and Roche. D.E. reports consulting fees from AstraZeneca, Daiichi Sankyo, Gilead, Lilly, Menarini, MSD, Novartis, Pfizer, Roche, Seagen and Sirius Medical; honoraria from AstraZeneca, Daiichi Sankyo, Gilead, Lilly, Menarini, MSD, Novartis, Pfizer, Roche, Seagen and Sirius Medical; meeting/travel support from Daiichi Sankyo and Pfizer; and receipt of medical writing support from Sirius Medical. F.A. reports being an employee of Bristol Myers Squibb. M.P. reports being an employee and shareholder of Bristol Myers Squibb. A.C. reports being an employee of Bristol Myers Squibb and shareholder of Merck. R.C. reports being an employee of Bristol Myers Squibb. R.N. reports being an employee and shareholder of Bristol Myers Squibb. T.S. reports being an employee and shareholder of Bristol Myers Squibb. J.Q.W. reports being an employee and shareholder of Bristol Myers Squibb. L.P. reports institutional research funding from AstraZeneca, Bristol Myers Squibb, GlaxoSmithKline, Merck, Pfizer and Seagen; consulting fees from AstraZeneca, Bristol Myers Squibb, Daiichi, Exact Sciences, Genentech-Roche, GlaxoSmithKline, Merck, Natera, Novartis, Personalis, Pfizer and Stemline-Menarini; and honoraria for advisory board participation from AstraZeneca, Bristol Myers Squibb, Daiichi, Exact Sciences, Genentech-Roche, GlaxoSmithKline, Merck, Natera, Novartis, Personalis, Pfizer and Stemline-Menarini. H.M. reports consulting fees from Amgen, AstraZeneca, Bristol Myers Squibb, Calithera, Celgene, Crown Bioscience Daiichi Sankyo, Lilly, Genentech-Roche, Gilead, Immunomedics, Merck, OBI Pharma, Peregrine, Pfizer, Puma, Spectrum Pharmaceuticals, Syndax Pharmaceuticals, Seattle Genetics and TapImmune; and research funding from Bristol Myers Squibb, BTG, LLC/AstraZeneca, MedImmune and Merck. R.I.R.D., A.S.Z., F.R.C., A.U. and J.G.R.-T. declare no competing interests.
Figures

References
-
- Jin, X. et al. Molecular classification of hormone receptor-positive HER2-negative breast cancer. Nat. Genet.55, 1696–1708 (2023). - PubMed
-
- Loibl, S. et al. Early breast cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol.35, 159–182 (2024). - PubMed
-
- Burstein, H. J., Lacchetti, C. & Griggs, J. J. Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: ASCO clinical practice guideline focused update. J. Oncol. Pract.15, 106–107 (2019). - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
