

Artificial intelligence assisted risk prediction in organ transplantation: a UK Live-Donor Kidney Transplant Outcome Prediction tool
- PMID: 39838510
- PMCID: PMC11755740
- DOI: 10.1080/0886022X.2024.2431147
Artificial intelligence assisted risk prediction in organ transplantation: a UK Live-Donor Kidney Transplant Outcome Prediction tool
Abstract
Introduction: Predicting the outcome of a kidney transplant involving a living donor advances donor decision-making donors for clinicians and patients. However, the discriminative or calibration capacity of the currently employed models are limited. We set out to apply artificial intelligence (AI) algorithms to create a highly predictive risk stratification indicator, applicable to the UK's transplant selection process.
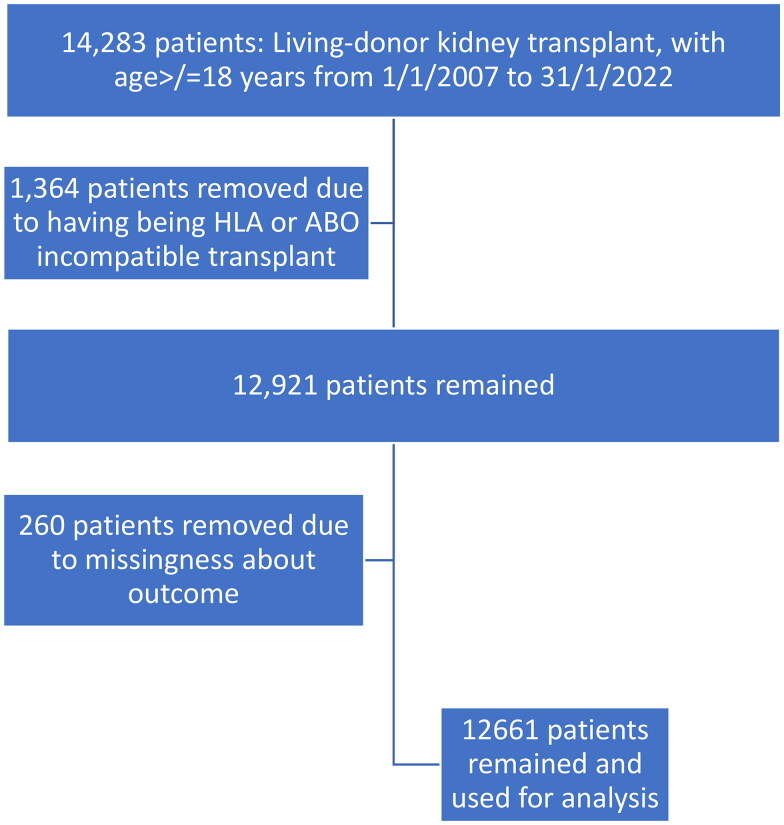
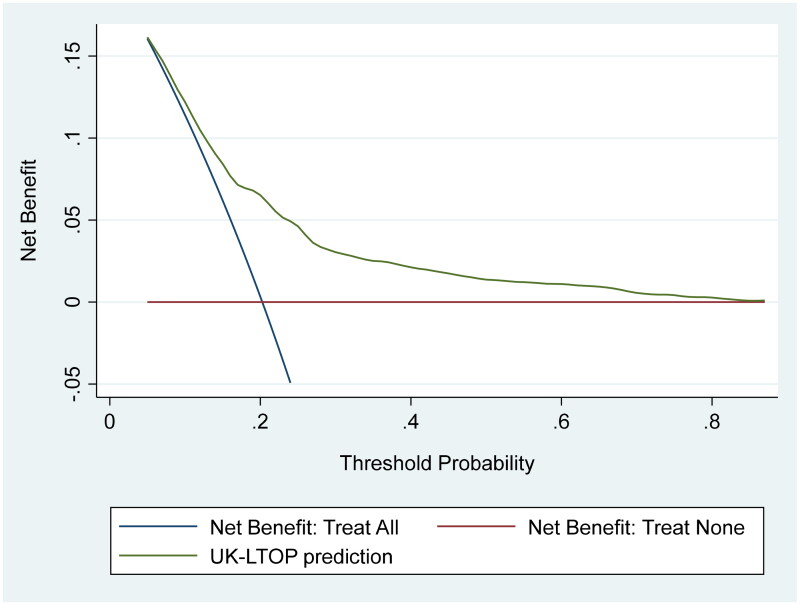
Methodology: Pre-transplant characteristics from 12,661 live-donor kidney transplants (performed between 2007 and 2022) from the United Kingdom Transplant Registry database were analyzed. The transplants were randomly divided into training (70%) and validation (30%) sets. Death-censored graft survival was the primary performance indicator. We experimented with four machine learning (ML) models assessed for calibration and discrimination [integrated Brier score (IBS) and Harrell's concordance index]. We assessed the potential clinical utility using decision curve analysis.
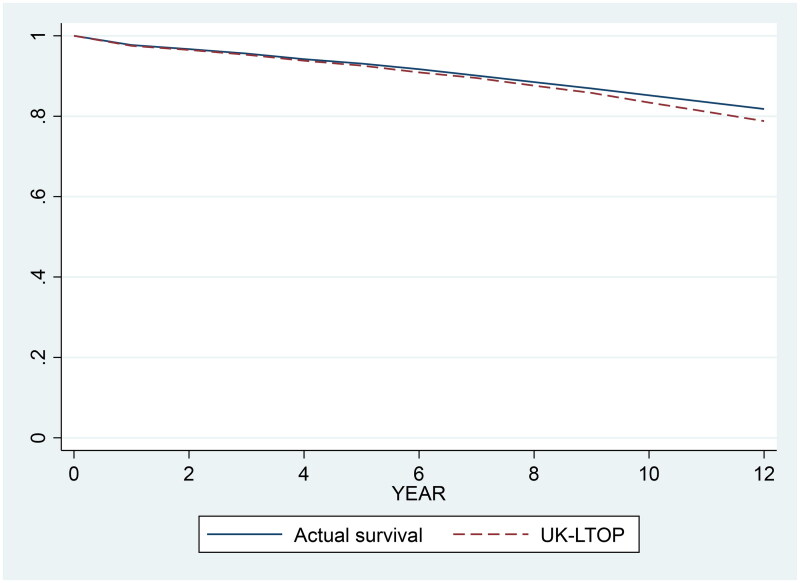
Results: XGBoost demonstrated the best discriminative performance for survival (area under the curve = 0.73, 0.74, and 0.75 at 3, 7, and 10 years post-transplant, respectively). The concordance index was 0.72. The calibration process was adequate, as evidenced by the IBS score of 0.09.
Conclusion: By evaluating possible donor-recipient pairs based on graft survival, the AI-based UK Live-Donor Kidney Transplant Outcome Prediction has the potential to enhance choices for the best live-donor selection. This methodology may improve the outcomes of kidney paired exchange schemes. In general terms we show how the new AI and ML tools can have a role in developing effective and equitable healthcare.
Keywords: Transplant outcomes; deceased kidney donor; machine learning; personalized medicine.
Plain language summary
Prior models for predicting outcomes in organ transplantation have limited discriminative and calibration power, highlighting a need for improved prediction tools that can better guide clinical decision-making.Differences in healthcare systems and data collection methodologies challenge the development of universally applicable predictive models for kidney transplantation outcomes.There is a recognized need for region-specific predictive models that take into account local healthcare practices and patient demographics to enhance transplant outcomes.
Conflict of interest statement
The authors declare that there are no conflicts of interest regarding the publication of this article. Dr. Fülöp is a current employee of the United States Veterans Health Administration. However, the views and opinions expressed herewith do not reflect the official views or opinions of and are not endorsed by the United States Veteran Health Administration. The authors confirm that none of the authors has been involved in the editorial handling or peer review. The authors confirm that no competing interests to declare.
Figures
Similar articles
-
Improved survival prediction for kidney transplant outcomes using artificial intelligence-based models: development of the UK Deceased Donor Kidney Transplant Outcome Prediction (UK-DTOP) Tool.Ren Fail. 2024 Dec;46(2):2373273. doi: 10.1080/0886022X.2024.2373273. Epub 2024 Oct 22. Ren Fail. 2024. PMID: 39437817 Free PMC article.
-
Live-Donor Kidney Transplant Outcome Prediction (L-TOP) using artificial intelligence.Nephrol Dial Transplant. 2024 Nov 27;39(12):2088-2099. doi: 10.1093/ndt/gfae088. Nephrol Dial Transplant. 2024. PMID: 38684469
-
Deceased-Donor Kidney Transplant Outcome Prediction Using Artificial Intelligence to Aid Decision-Making in Kidney Allocation.ASAIO J. 2024 Sep 1;70(9):808-818. doi: 10.1097/MAT.0000000000002190. Epub 2024 Mar 29. ASAIO J. 2024. PMID: 38552178
-
Four years of experience with the Australian kidney paired donation programme.Nephrology (Carlton). 2015 Mar;20(3):124-31. doi: 10.1111/nep.12369. Nephrology (Carlton). 2015. PMID: 25408125 Review.
-
Using Artificial Intelligence for Predicting Survival of Individual Grafts in Liver Transplantation: A Systematic Review.Liver Transpl. 2020 Jul;26(7):922-934. doi: 10.1002/lt.25772. Epub 2020 Jun 23. Liver Transpl. 2020. PMID: 32274856
Cited by
-
Optimizing Tacrolimus Dosing During Hospitalization After Kidney Transplantation: A Comparative Model Analysis.Ann Transplant. 2025 Apr 1;30:e947768. doi: 10.12659/AOT.947768. Ann Transplant. 2025. PMID: 40165354 Free PMC article.
-
Artificial Intelligence-Driven Drug Toxicity Prediction: Advances, Challenges, and Future Directions.Toxics. 2025 Jun 23;13(7):525. doi: 10.3390/toxics13070525. Toxics. 2025. PMID: 40710970 Free PMC article. Review.
-
Development of explainable artificial intelligence based machine learning model for predicting 30-day hospital readmission after renal transplantation.BMC Nephrol. 2025 Apr 22;26(1):203. doi: 10.1186/s12882-025-04128-w. BMC Nephrol. 2025. PMID: 40264055 Free PMC article.
References
-
- Cecka JM. Living donor transplants. In: Cecka JM, Terasaki PI, editors. Clinical transplants. Los Angeles: U.C.L.A. Tissue Typing Laboratory; 1995.p. 363. - PubMed
-
- Rapaport FT. The case for a living emotionally related international kidney donor exchange registry. Transplant Proc. 1986;18(3 Suppl. 2):5–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical