

Prediction and stratification for the surgical adverse events after minimally invasive esophagectomy: A two-center retrospective study
- PMID: 39839907
- PMCID: PMC11684167
- DOI: 10.3748/wjg.v31.i3.101041
Prediction and stratification for the surgical adverse events after minimally invasive esophagectomy: A two-center retrospective study
Abstract
Background: Minimally invasive esophagectomy (MIE) is a widely accepted treatment for esophageal cancer, yet it is associated with a significant risk of surgical adverse events (SAEs), which can compromise patient recovery and long-term survival. Accurate preoperative identification of high-risk patients is critical for improving outcomes.
Aim: To establish and validate a risk prediction and stratification model for the risk of SAEs in patients with MIE.
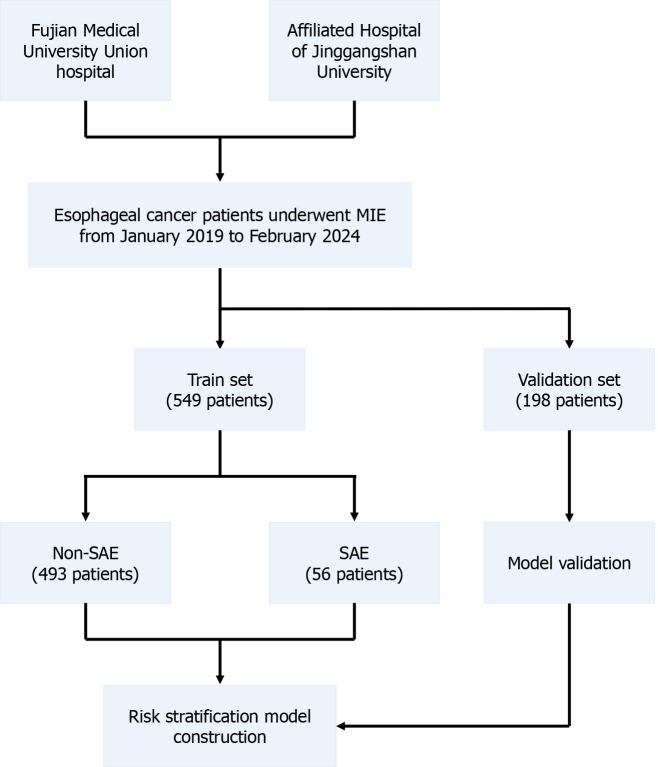
Methods: This retrospective study included 747 patients who underwent MIE at two centers from January 2019 to February 2024. Patients were separated into a train set (n = 549) and a validation set (n = 198). After screening by least absolute shrinkage and selection operator regression, multivariate logistic regression analyzed clinical and intraoperative variables to identify independent risk factors for SAEs. A risk stratification model was constructed and validated to predict the probability of SAEs.
Results: SAEs occurred in 10.2% of patients in train set and 13.6% in the validation set. Patients with SAE had significantly higher complication rate and a longer hospital stay after surgery. The key independent risk factors identified included chronic obstructive pulmonary disease, a history of alcohol consumption, low forced expiratory volume in the first second, and low albumin levels. The stratification model has excellent prediction accuracy, with an area under the curve of 0.889 for the training set and an area under the curve of 0.793 for the validation set.
Conclusion: The developed risk stratification model effectively predicts the risk of SAEs in patients undergoing MIE, facilitating targeted preoperative interventions and improving perioperative management.
Keywords: Esophageal cancer; Minimally invasive esophagectomy; Perioperative management; Stratification model; Surgical adverse events.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures






References
-
- Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229–263. - PubMed
-
- Low DE, Kuppusamy MK, Alderson D, Cecconello I, Chang AC, Darling G, Davies A, D'Journo XB, Gisbertz SS, Griffin SM, Hardwick R, Hoelscher A, Hofstetter W, Jobe B, Kitagawa Y, Law S, Mariette C, Maynard N, Morse CR, Nafteux P, Pera M, Pramesh CS, Puig S, Reynolds JV, Schroeder W, Smithers M, Wijnhoven BPL. Benchmarking Complications Associated with Esophagectomy. Ann Surg. 2019;269:291–298. - PubMed
-
- Kalata S, Singh B, Graham N, Fan Z, Chang AC, Lynch WR, Lagisetty KH, Lin J, Yeung J, Reddy RM, Wakeam E. Epidemiology of Postoperative Complications After Esophagectomy: Implications for Management. Ann Thorac Surg. 2023;116:1168–1175. - PubMed
-
- Deana C, Vetrugno L, Stefani F, Basso A, Matellon C, Barbariol F, Vecchiato M, Ziccarelli A, Valent F, Bove T, Bassi F, Petri R, De Monte A. Postoperative complications after minimally invasive esophagectomy in the prone position: any anesthesia-related factor? Tumori. 2021;107:525–535. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
