

Association of prostate-specific antigen density with prostate cancer mortality after a benign systematic prostate biopsy result
- PMID: 39840544
- PMCID: PMC11975165
- DOI: 10.1111/bju.16641
Association of prostate-specific antigen density with prostate cancer mortality after a benign systematic prostate biopsy result
Abstract
Objective: To assess the association between prostate-specific antigen (PSA) density (PSAD) and prostate cancer mortality after a benign result on systematic transrectal ultrasonography (TRUS)-guided prostate biopsy.
Patients and methods: This retrospective study used data from the Finnish Randomised Study of Screening for Prostate Cancer (FinRSPC) collected between 1996 and 2020. We identified men aged 55-71 years randomised to the screening arm with PSA ≥4.0 ng/mL and a benign systematic TRUS-guided biopsy result. The cumulative prostate cancer mortality of men stratified by a PSAD cutoff of 0.15 ng/mL/cm3 was modelled with competing risk functions. The ability of PSAD, PSA, and base variables (age at biopsy, DRE result, socioeconomic status, 5α-reductase inhibitor usage, family history, and Charlson Comorbidity Index (CCI)) to predict prostate cancer death was compared using c-statistics and a likelihood ratio test.
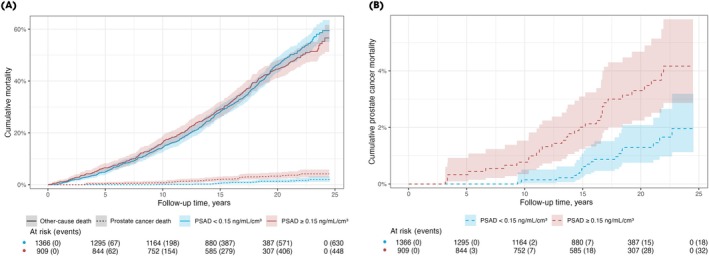
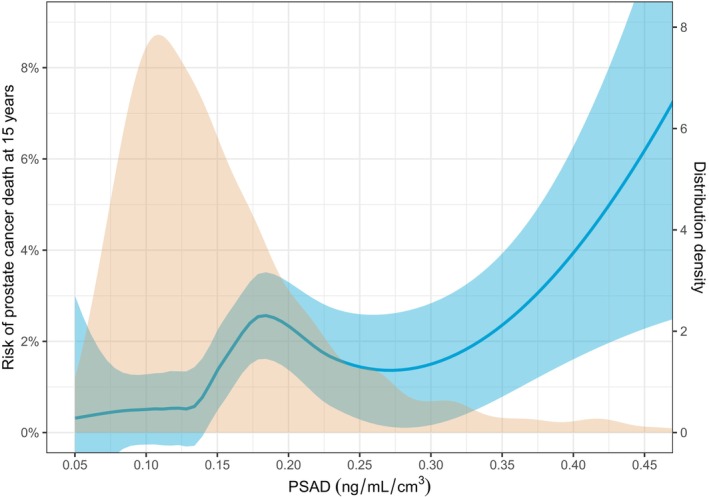
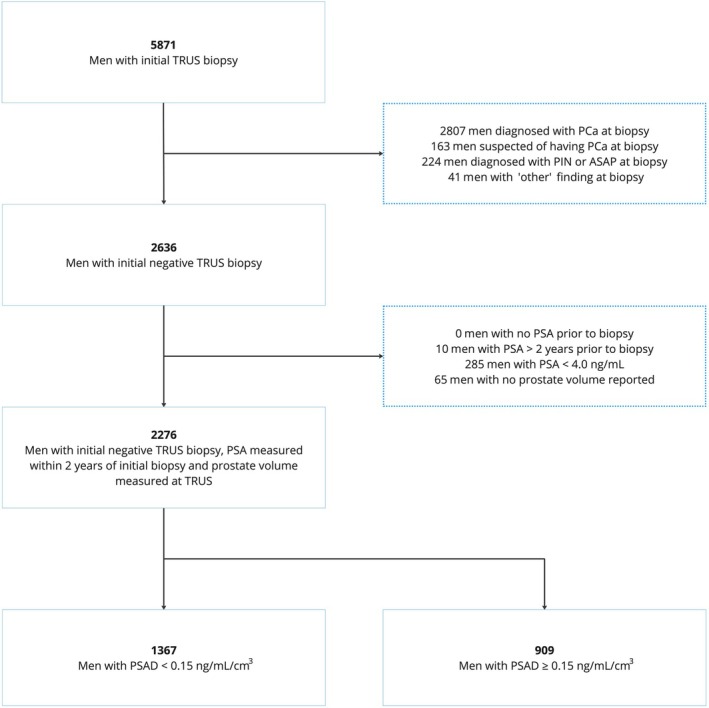
Results: After excluding 10 men without PSA data within 2 years of the biopsy and 65 without prostate volume data, 2276 men were eligible for inclusion in the study. A total of 50 men died from prostate cancer and 1028 from other causes during a median (interquartile range) follow-up of 17.4 (13.2-20.9) years. The cumulative prostate cancer mortality of men with PSAD <0.15 ng/mL/cm3 was significantly lower than that of men with PSAD ≥0.15 ng/mL/cm3: 0.5% (95% confidence interval [CI] 0.2%-1.1%) vs 2.0% (95% CI 1.2%-3.1%) at 15 years (Grey's test, P = 0.001). The model consisting of PSAD, PSA and the base variables predicted prostate cancer mortality (c-statistic 0.781) significantly better than either the base variables alone (c-statistic 0.737; likelihood-ratio test, P = 0.003) or the base variables and PSA (c-statistic 0.765; likelihood-ratio test, P = 0.039).
Conclusion: Prostate cancer mortality after a benign systematic TRUS-guided biopsy is low. In these patients, PSAD predicts prostate cancer mortality and provides additional value to other clinical variables. PSAD-based stratification can be used to guide follow-up strategy.
Keywords: comparative study; follow‐up; prostate biopsy; prostate cancer; prostate‐specific antigen density.
© 2025 The Author(s). BJU International published by John Wiley & Sons Ltd on behalf of BJU International.
Figures
Similar articles
-
Detection of prostate carcinoma using prostate specific antigen, its density, and the density of the transition zone in Japanese men with intermediate serum prostate specific antigen concentrations.Cancer. 1997 May 15;79(10):1969-76. doi: 10.1002/(sici)1097-0142(19970515)79:10<1969::aid-cncr19>3.0.co;2-t. Cancer. 1997. PMID: 9149025
-
Volume-adjusted prostate-specific antigen (PSA) variables in detecting impalpable prostate cancer in men with PSA levels of 2-4 ng/mL: transabdominal measurement makes a significant contribution.BJU Int. 2005 Jun;95(9):1245-8. doi: 10.1111/j.1464-410X.2005.05513.x. BJU Int. 2005. PMID: 15892809
-
An algorithm for prostate cancer detection in a patient population using prostate-specific antigen and prostate-specific antigen density.World J Urol. 1993;11(4):206-13. doi: 10.1007/BF00185070. World J Urol. 1993. PMID: 7508785
-
Evaluation of prostate specific antigen density and transrectal ultrasonography-guided biopsies in 100 consecutive patients with a negative digital rectal examination and intermediate serum prostate specific antigen levels.Int J Urol. 1997 Jul;4(4):362-7. doi: 10.1111/j.1442-2042.1997.tb00209.x. Int J Urol. 1997. PMID: 9256325 Review.
-
Predictive factors of incidental prostate cancer in patients undergoing surgery for presumed benign prostatic hyperplasia: an updated systematic review and meta-analysis.Front Oncol. 2025 Feb 27;15:1561675. doi: 10.3389/fonc.2025.1561675. eCollection 2025. Front Oncol. 2025. PMID: 40083876 Free PMC article.
References
-
- EAU Guidelines . Edn. presented at the EAU annual congress Milan 2023. ISBN 978‐94‐92671‐19‐6
-
- Drost FH, Osses D, Nieboer D et al. Prostate magnetic resonance imaging, with or without magnetic resonance imaging‐targeted biopsy, and systematic biopsy for detecting prostate cancer: a Cochrane systematic review and meta‐analysis. Eur Urol 2020; 77: 78–94 - PubMed
-
- Sayyid RK, Alibhai SMH, Sutradhar R et al. Population‐based outcomes of men with a single negative prostate biopsy: importance of continued follow‐up among older patients. Urol Oncol 2019; 37: 298.e19–27 - PubMed
-
- Palmstedt E, Månsson M, Frånlund M et al. Long‐term outcomes for men in a prostate screening trial with an initial benign prostate biopsy: a population‐based cohort. Eur Urol Oncol 2019; 2: 716–722 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
