

Effects of Continuous Graduated Pneumatic Compression and Intermittent Pneumatic Compression on Lower Limb Hemodynamics for VTE Prophylaxis in Arthroplasty
- PMID: 39840650
- PMCID: PMC11962296
- DOI: 10.1111/os.14360
Effects of Continuous Graduated Pneumatic Compression and Intermittent Pneumatic Compression on Lower Limb Hemodynamics for VTE Prophylaxis in Arthroplasty
Abstract
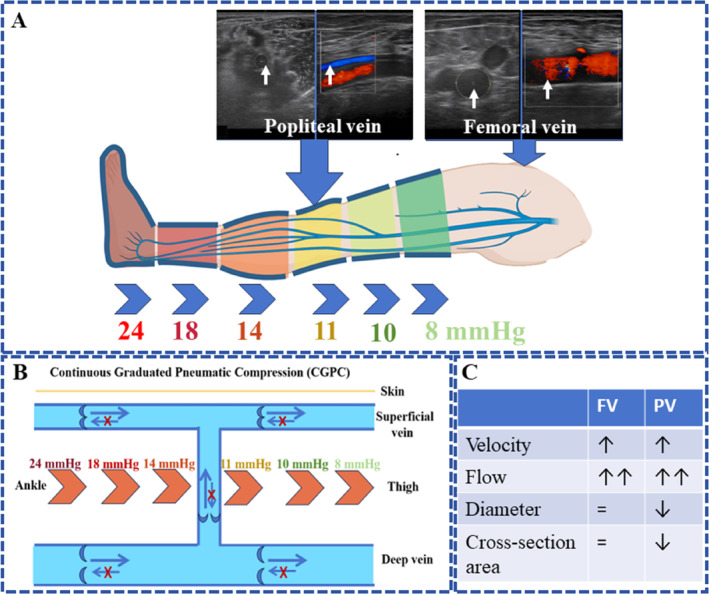
Objective: Intermittent pneumatic compression (IPC) is considered the standard of care for preventing venous thromboembolism (VTE) in the hospital setting. However, its widespread adoption after hospitalization has been limited due to its shortcomings in obstruction of venous valves and blood reflux. The objective of this study is to compare the effects of continuous graduated pneumatic compression (CGPC), a new device with a novel mechanism, and IPC on lower hemodynamics and the incidence of VTE in patients undergoing arthroplasty.
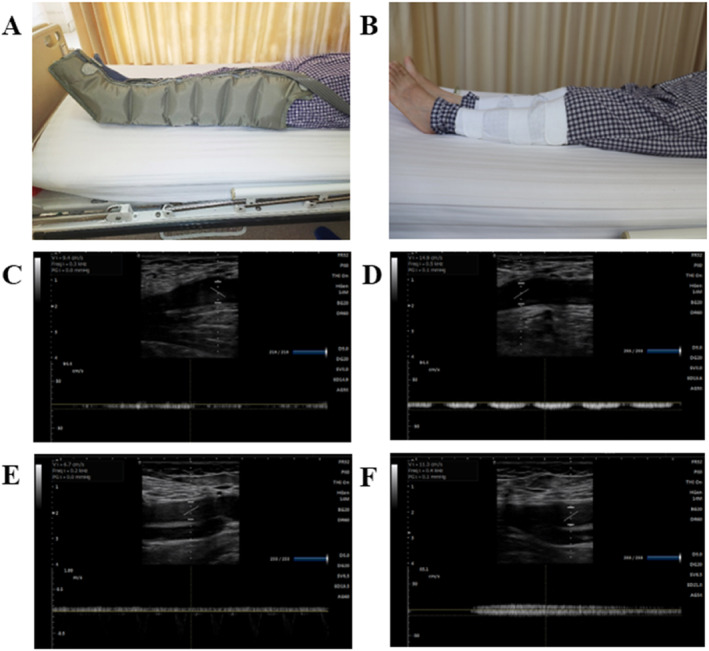
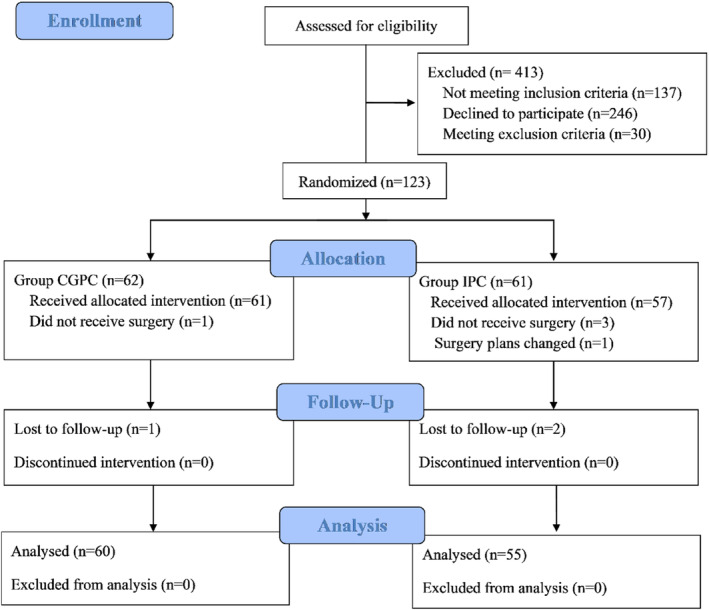
Methods: We randomized 123 participants undergoing knee arthroplasty to receive either IPC or CGPC from June 2022 through August 2023. An experienced sonographer used a Doppler ultrasound scanner to obtain hemodynamic indicators of venous blood. The primary outcome was the blood velocity of the femoral vein measured by a Doppler scanner. Secondary outcomes included the hemodynamic of the femoral vein and popliteal vein, quality of life at discharge and 30 days after surgery, symptomatic and asymptomatic VTE up to 30 days, and adverse events related to the IPC and CGPC device. For statistical analyses, Student's t-test, analysis of covariance, and the Mann-Whitney U test were used. Statistical significance was indicated with p < 0.05.
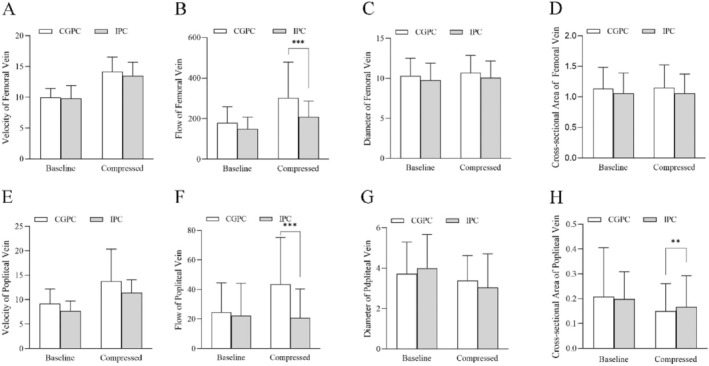
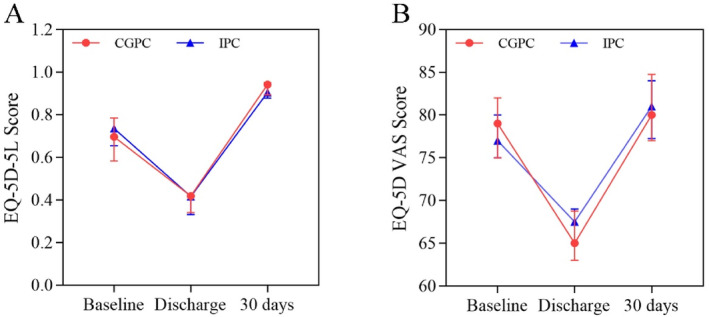
Results: There was no significant difference in femoral vein velocity between the IPC and CGPC groups. However, CGPC demonstrated a significant increase in femoral vein flow compared to the IPC group, with a median (interquartile) increasing from 158.9 (122.9, 204.3) to 265.6 (203.3, 326.8) mL/min in the CGPC group and from 139.0 (103.3, 175.9) to 189.6 (161.4, 270.8) mL/min in the IPC group (p < 0.001). Similar trends were observed in popliteal vein measurements. The differences between the two groups were similar in terms of quality of life, incidence of VTE, and adverse events.
Conclusion: The CGPC device provides a substantial increase in blood flow compared to the IPC device. Its safety and effectiveness have been preliminarily validated. The CGPC device presents a promising alternative for VTE prophylaxis in arthroplasty.
Trial registration: Chinese Clinical Trial Registry (registration number: ChiCTR2300078201).
Keywords: arthroplasty; continuous graduated pneumatic compression; hemodynamics; intermittent pneumatic compression; venous thromboembolism.
© 2025 The Author(s). Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Different types of intermittent pneumatic compression devices for preventing venous thromboembolism in patients after total hip replacement.Cochrane Database Syst Rev. 2012 Nov 14;11:CD009543. doi: 10.1002/14651858.CD009543.pub2. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2014 Dec 22;(12):CD009543. doi: 10.1002/14651858.CD009543.pub3. PMID: 23152279 Updated.
-
Combined intermittent pneumatic leg compression and pharmacological prophylaxis for prevention of venous thromboembolism.Cochrane Database Syst Rev. 2022 Jan 28;1(1):CD005258. doi: 10.1002/14651858.CD005258.pub4. Cochrane Database Syst Rev. 2022. PMID: 35089599 Free PMC article.
-
Different types of intermittent pneumatic compression devices for preventing venous thromboembolism in patients after total hip replacement.Cochrane Database Syst Rev. 2014 Dec 22;2014(12):CD009543. doi: 10.1002/14651858.CD009543.pub3. Cochrane Database Syst Rev. 2014. PMID: 25528992 Free PMC article.
-
Meta-Analysis of the Role of Intermittent Pneumatic Compression of the Lower Limbs to Prevent Venous Thromboembolism in Critically Ill Patients.Int J Low Extrem Wounds. 2022 Mar;21(1):31-40. doi: 10.1177/1534734620925391. Epub 2020 Jun 11. Int J Low Extrem Wounds. 2022. PMID: 32527203
-
Neuromuscular electrical stimulation for the prevention of venous thromboembolism.Cochrane Database Syst Rev. 2017 Nov 21;11(11):CD011764. doi: 10.1002/14651858.CD011764.pub2. Cochrane Database Syst Rev. 2017. PMID: 29161465 Free PMC article.
References
-
- Cohen A. T., Tapson V. F., Bergmann J. F., et al., “Venous Thromboembolism Risk and Prophylaxis in the Acute Hospital Care Setting (ENDORSE Study): A Multinational Cross‐Sectional Study,” Lancet 371, no. 9610 (2008): 387–394. - PubMed
-
- Amanatullah D. F., Shah H. N., Johnson B., and Wall J., “Mechanical Compression Augments Venous Flow Equal to Intermittent Pneumatic Compression,” Journal of Orthopaedic Research 38, no. 11 (2020): 2390–2395. - PubMed
-
- Bahl V., Hu H. M., Henke P. K., Wakefield T. W., D. A. Campbell, Jr. , and Caprini J. A., “A Validation Study of a Retrospective Venous Thromboembolism Risk Scoring Method,” Annals of Surgery 251, no. 2 (2010): 344–350. - PubMed
-
- Caprini J. A., Arcelus J. I., Hasty J. H., Tamhane A. C., and Fabrega F., “Clinical Assessment of Venous Thromboembolic Risk in Surgical Patients,” Seminars in Thrombosis and Hemostasis 17, no. Suppl 3 (1991): 304–312. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
