

Intradural Disk Herniation at the Conus Medullaris: A Case Report With Emphasis on Patient Positioning and Neuromonitoring
- PMID: 39841040
- PMCID: PMC11581431
- DOI: 10.2106/JBJS.CC.24.00235
Intradural Disk Herniation at the Conus Medullaris: A Case Report With Emphasis on Patient Positioning and Neuromonitoring
Erratum in
-
Erratum: Intradural Disk Herniation at the Conus Medullaris: A Case Report With Emphasis on Patient Positioning and Neuromonitoring.JBJS Case Connect. 2025 Jan 24;15(1):e24.00235ER. doi: 10.2106/JBJS.CC.ER.24.00235. eCollection 2025 Jan 1. JBJS Case Connect. 2025. PMID: 39854544 Free PMC article. No abstract available.
Abstract
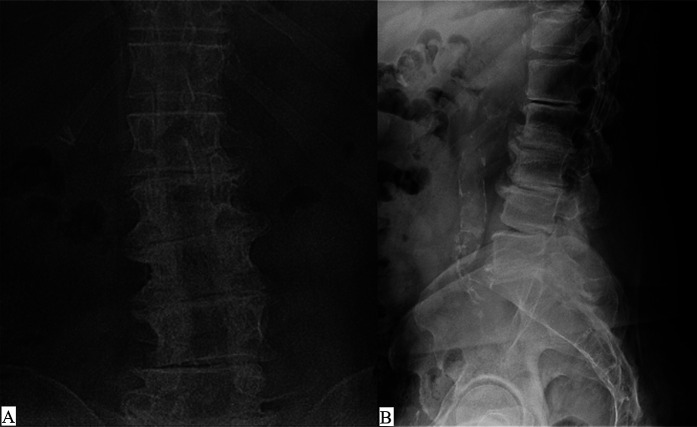
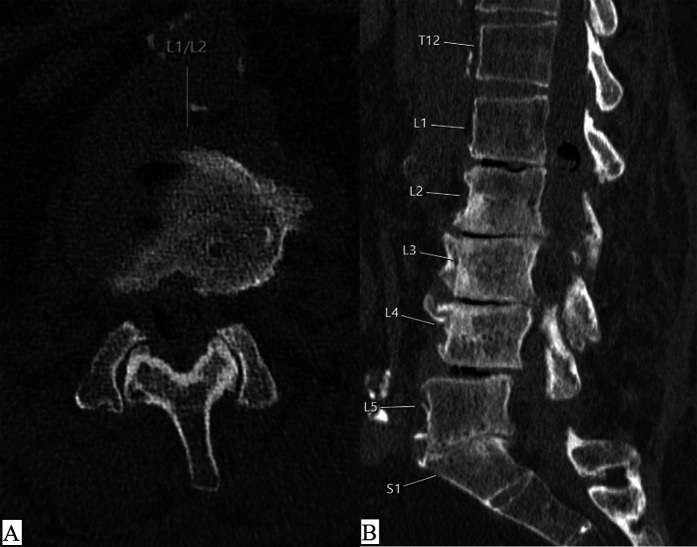
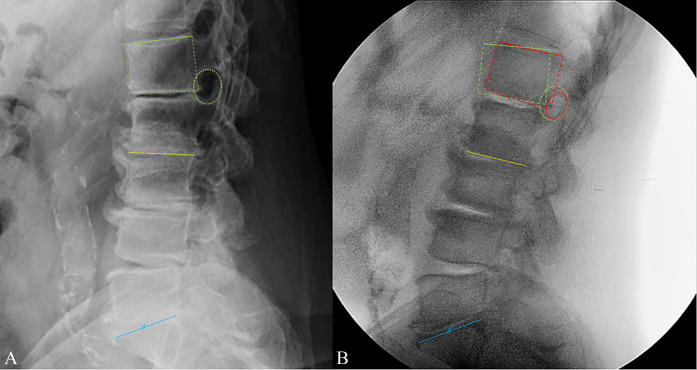
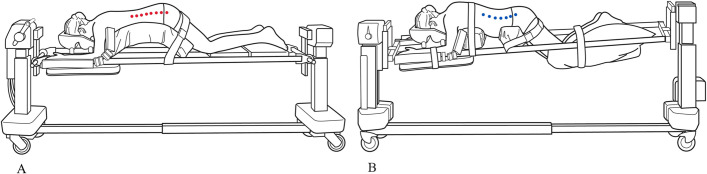
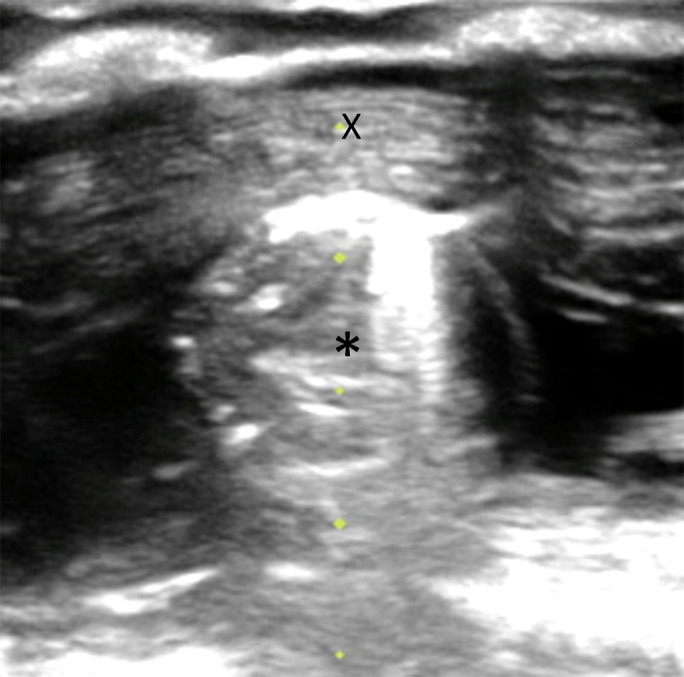
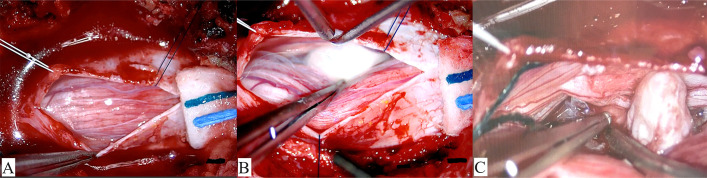
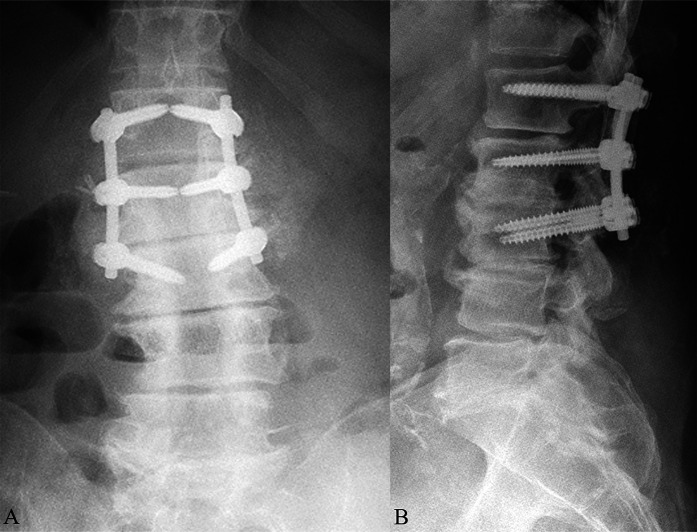
Case: A 73-year old man who underwent previous L2-S1 decompression presenting with new right radicular leg pain. Imaging suggests a large central disk herniation at L1-2 with possible intrathecal extension requiring surgical decompression. When positioned prone on a Jackson frame, neuromonitoring motor signals became diminished, and thus, the case was aborted. On returning to the operating room 2 days later, careful positioning in a more neutral/flexed position facilitated normal neuromonitoring signals, allowing for an uneventful intradural approach and discectomy.
Conclusion: With conus-level intrathecal disk herniation, consider using prepositional neuromonitoring and avoid hyperextension with positioning to ensure neurological safety.
Copyright © 2024 The Authors. Published by The Journal of Bone and Joint Surgery, Incorporated.
Conflict of interest statement
Disclosure: The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article (http://links.lww.com/JBJSCC/C486).
Figures

References
-
- Deyo RA, Mirza SK. CLINICAL PRACTICE. herniated lumbar intervertebral disk. N Engl J Med. 2016;374(18):1763-72. - PubMed
-
- Dandy WE. Serious complications of ruptured intervertebral disks. JAMA. 1942;119(6):474-7.
-
- Hu X, Chang W. An unusual case report of intradural disc herniation mimicking the spinal intradural tumor. Asian J Surg. 2023;46(12):5546-7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
