

Ileal pouch-anal anastomosis for ulcerative colitis: 30-year analysis on surgical evolution and patient outcome
- PMID: 39841130
- PMCID: PMC11752858
- DOI: 10.1093/bjsopen/zrae111
Ileal pouch-anal anastomosis for ulcerative colitis: 30-year analysis on surgical evolution and patient outcome
Abstract
Background: Proctocolectomy with ileal pouch-anal anastomosis is the treatment of choice for patients with ulcerative colitis with medical refractory disease or dysplasia. The aim of this research was to describe the evolution of ileal pouch-anal anastomosis surgery and surgical outcomes over a three-decade interval in a high-volume referral centre.
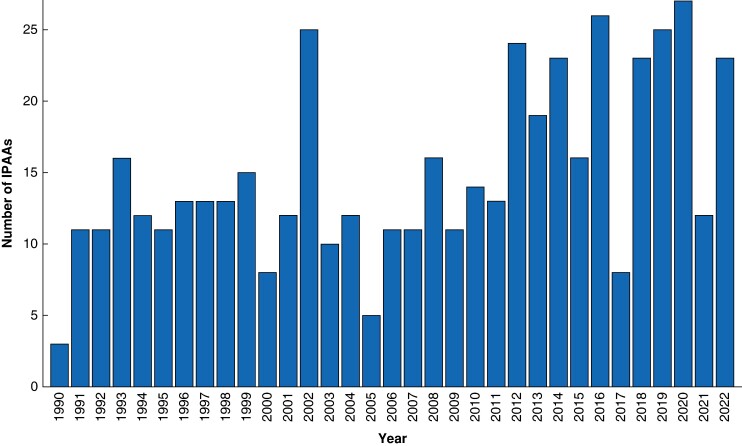
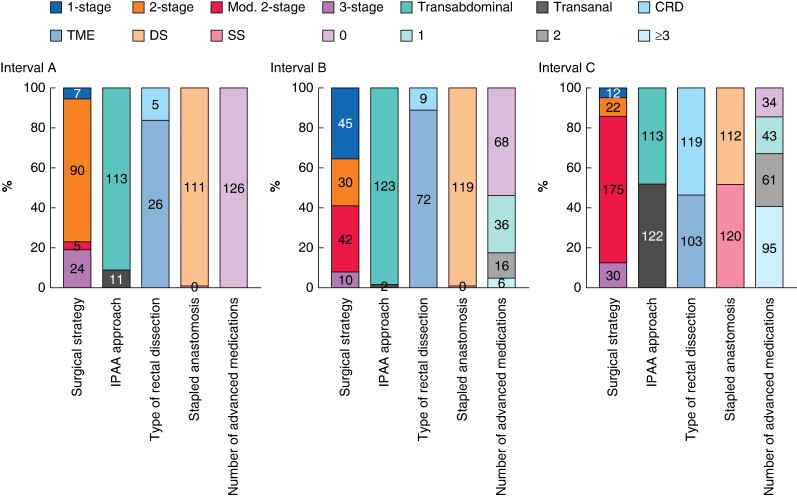
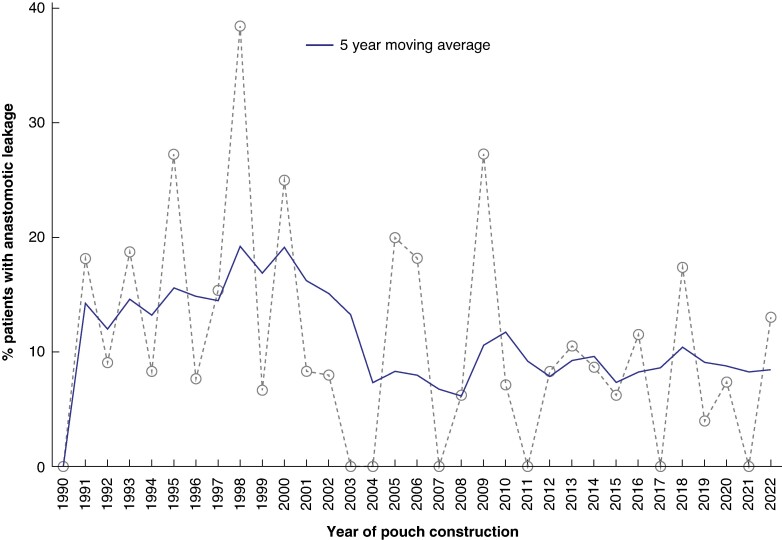
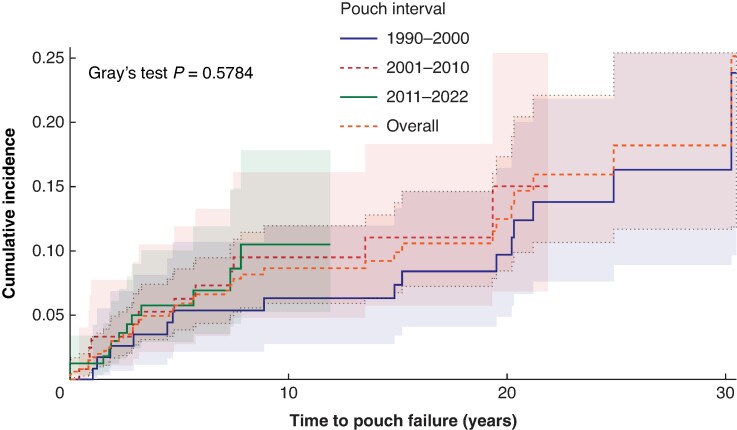
Methods: All consecutive patients undergoing ileal pouch-anal anastomosis for ulcerative colitis between 1990 and 2022 at the University Hospitals of Leuven were retrospectively included. Patients were divided into three interval arms (interval A 1990-2000, interval B 2001-2010 and interval C 2011-2022). The primary outcomes of interest were anastomotic leakage at 30 days and pouch failure.
Results: Overall, 492 patients were included. The use of preoperative advanced therapies increased over time (P < 0.001). An increase in laparoscopic procedures (23.2% in interval A, 66.4% in interval B, 86.0% in interval C; P < 0.001) and a shift towards delayed ileal pouch-anal anastomosis (colectomy-first approach with delayed ileal pouch-anal anastomosis construction: 23.0% in interval A, 40.9% in interval B, 85.8% in interval C; P < 0.001) were observed. Anastomotic leakage rate decreased from 16.7% (interval A) to 8.4% (interval C) (P = 0.04). Delayed ileal pouch-anal anastomosis was the most relevant factor in limiting leakage (OR 0.49 (95% c.i. 0.27 to 0.87); P = 0.016). Median follow-up was 7.5 years (interquartile range 2.5-16). Cumulative pouch failure incidence was 8.2%, not significantly different between the three intervals (P = 0.580). Anastomotic leakage was the only significant risk factor for pouch failure (HR 2.82 (95% c.i. 1.29 to 6.20); P = 0.010).
Conclusion: Significant changes in the management of ulcerative colitis patients occurred. Despite the widespread use of advanced therapies and the expanded surgical indications, anastomotic leakage rate decreased over time. In the context of a delayed ileal pouch-anal anastomosis, diverting ileostomy could be avoided in selected cases. Anastomotic leakage remains the most relevant risk factor for pouch failure. Pouch failure incidence remained stable over the years.
© The Author(s) 2025. Published by Oxford University Press on behalf of BJS Foundation Ltd.
Figures
References
-
- Dayton MT, Larsen KP. Outcome of pouch-related complications after ileal pouch-anal anastomosis. Am J Surg 1997;174:728–731; discussion 731–2 - PubMed
-
- Baek SJ, Dozois EJ, Mathis KL, Lightner AL, Boostrom SY, Cima RR et al. Safety, feasibility, and short-term outcomes in 588 patients undergoing minimally invasive ileal pouch-anal anastomosis: a single-institution experience. Tech Coloproctol 2016;20:369–374 - PubMed
-
- Geltzeiler CB, Lu KC, Diggs BS, Deveney KE, Keyashian K, Herzig DO et al. Initial surgical management of ulcerative colitis in the biologic era. Dis Colon Rectum 2014;57:1358–1363 - PubMed
-
- Bach SP, Mortensen NJ. Revolution and evolution: 30 years of ileoanal pouch surgery. Inflamm Bowel Dis 2006;12:131–145 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
