

The effects of ultra-selective beta1-antagonism on the metabolic and cytokine profile in septic shock patients receiving noradrenaline: a sub-investigation from the STRESS-L Randomised Study
- PMID: 39841388
- PMCID: PMC11754546
- DOI: 10.1186/s40635-024-00708-6
The effects of ultra-selective beta1-antagonism on the metabolic and cytokine profile in septic shock patients receiving noradrenaline: a sub-investigation from the STRESS-L Randomised Study
Abstract
Purpose: The landiolol and organ failure in patients with septic shock (STRESS-L study) included a pre-planned sub-study to assess the effect of landiolol treatment on inflammatory and metabolomic markers.
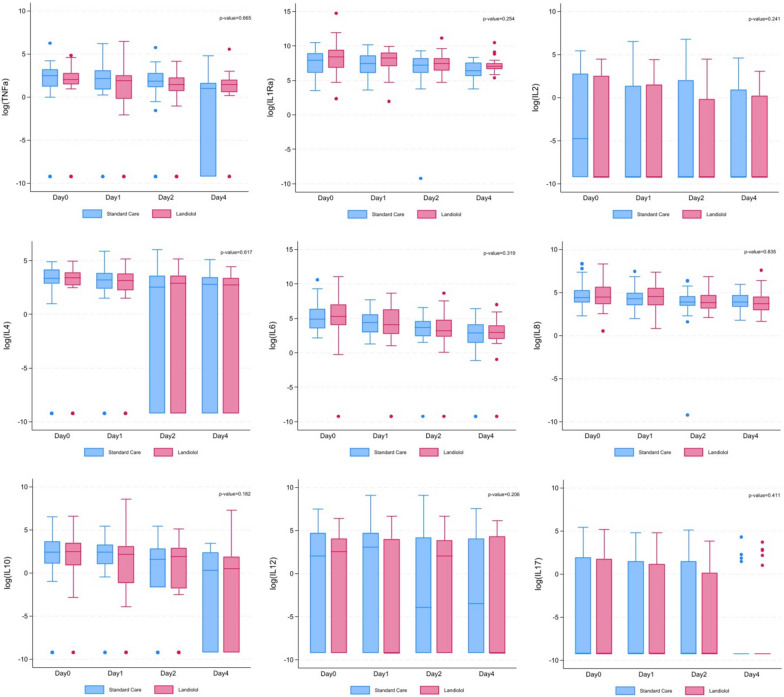
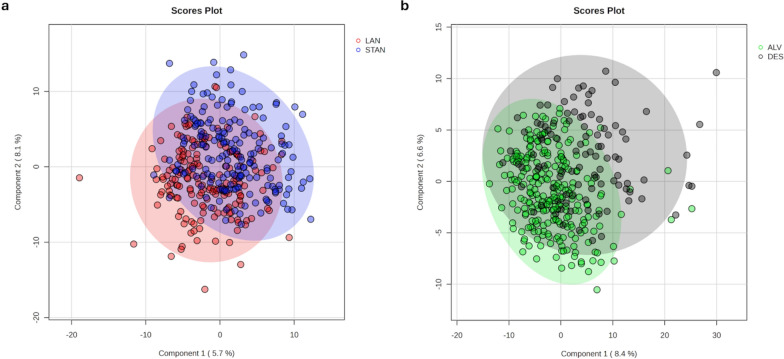
Methods: Samples collected from 91 patients randomised to STRESS-L were profiled for immune and metabolomic markers. A panel of pro- and anti-inflammatory cytokines were measured through commercially acquired multiplex Luminex assays and statistically analysed by individual and cluster-level analysis (patient). Metabolite fingerprinting was carried out by flow infusion electrospray ionisation high-resolution mass spectrometry and metabolomic data were analysed using the R-based platform MetaboAnalyst. The metabolites were identified using DIMEdb (dimedb.ibers.aber.ac.uk) from their mass/charge ratios. These metabolomic data were also re-analysed using individual and cluster-level analysis. The individual-level models were adjusted for confounders, such as age, sex, noradrenaline dosage and patient (random effect).
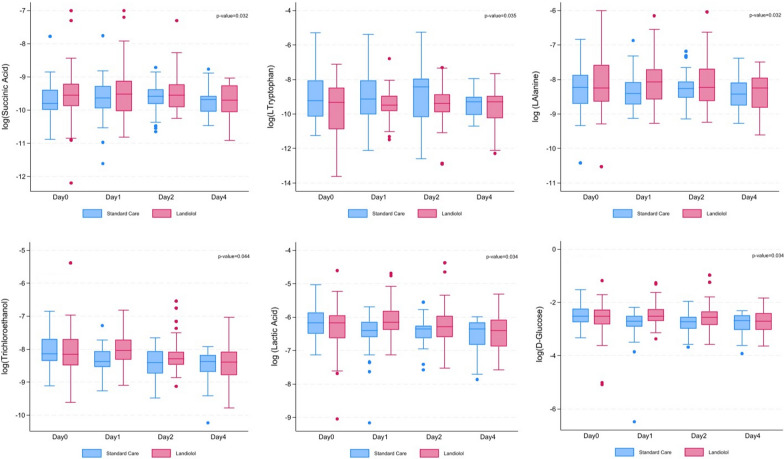
Results: Analysis was undertaken at cluster- and individual-level. There were no significant differences in cytokine concentration level between trial arms nor survivors and non-survivors over the duration of the observations from day 1 to day 4. Metabolomic analysis showed some separation in the levels of ceramides and cardiolipins between those who survived and those who died. Following adjusted analysis for confounders, plasma metabolite concentrations remained statistically different between landiolol and standard care arms for succinic acid, L-tryptophan, L-alanine, 2,2,2-trichloroethanol, lactic acid and D-glucose.
Conclusions: In a study of ICU patients with established septic shock and a tachycardia, landiolol treatment used to reduce the heart rate from above 95 to a range between 80 and 94 beats per minute did not induce significant cytokine changes. D-Glucose, lactic acid, succinic acid, L-alanine, L-tryptophan and trichloroethanol were pathways that may merit further investigation.
Trial registration: EU Clinical Trials Register Eudra CT: 2017-001785-14 ( https://www.clinicaltrialsregister.eu/ctr-search/trial/2017-001785-14/GB ); ISRCTN registry Identifier: ISRCTN12600919 ( https://www.isrctn.com/ISRCTN12600919 ).
Keywords: Clinical trial; Cytokines; Metabolomics; STRESS-L; Sepsis; Septic shock; β-Blocker.
© 2025. Crown.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The protocol for STRESS-L has been previously published [17] and was approved by the East of England, Essex Research Ethics Committee (Reference, 17/EE/0368). Consent for publication: No patient identity is revealed in the paper. Competing interests: Prof Whitehouse was the Chief Investigator for STRESS‐L which was funded by the National Institute for Health Research (NIHR) Efficacy and Mechanism Evaluation (Project Number: EME‐14/150/85) and during the conduct of the study, he received personal fees and non‐financial support from AOP Orphan, manufacturer of landiolol. Prof Perkins reported receiving grants from the Academic Research Collaboration West Midlands. Prof Gordon reported receiving grant RP-2015-06-18 from the National Institute for Health Research (NIHR); nonfinancial support from the NIHR Imperial Biomedical Research Centre (BRC) and the NIHR Clinical Research Network; and consulting fees paid to his institution from AstraZeneca, Janssen, and Novartis. Prof McAuley reported receiving grants from the NIHR, Wellcome Trust, Innovate UK, MRC, and the Northern Ireland Health and Social Care Research and Development Division; consulting fees from Aptarion, Aviceda, Bayer, Boehringer Ingelheim, Direct Biologics, Eli Lilly, GlaxoSmithKline, and Novartis; personal fees from Vir Biotechnology Inc; being a member of the Disability Management Employer Coalition, having patent US8962032 issued to Queen’s University Belfast; and serving as the codirector of research for the Intensive Care Society and director of the NIHR/MRC EME Programme. Prof Singer reported receiving grants to his institution from DSTL and Gentian, lecture fees from AOP Health, and serving on advisory boards for Aptarian, Biotest, deePull, Deltex Medical, Matisse, Pfizer, Roche, Safeguard and Volition. Prof Lord reported receiving grants from NIHR. The other authors declare no conflict of interest.
Figures
References
-
- Morelli A, Ertmer C, Westphal M, Rehberg S, Kampmeier T, Ligges S, Orecchioni A, D’Egidio A, D’Ippoliti F, Raffone C, Venditti M, Guarracino F, Girardis M, Tritapepe L, Pietropaoli P, Mebazaa A, Singer M (2013) Effect of heart rate control with esmolol on hemodynamic and clinical outcomes in patients with septic shock: a randomized clinical trial. JAMA 310:1683–1691 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
