

The paradoxical GH response at OGTT does not predict Pasireotide efficacy but matters for glucose metabolism
- PMID: 39841390
- PMCID: PMC12049373
- DOI: 10.1007/s40618-025-02534-3
The paradoxical GH response at OGTT does not predict Pasireotide efficacy but matters for glucose metabolism
Abstract
Purpose: A paradoxical increase in GH after oral glucose load (GH-Par) characterizes about one-third of acromegaly patients and is associated with a better response to first-generation somatostatin receptor ligands (fg-SRLs). Pasireotide is typically considered as a second-/third-line treatment. Here, we investigated the predictive role of GH-Par in pasireotide response and adverse event development.
Methods: we collected a multicenter Italian retrospective cohort of 59 patients treated with pasireotide for at least 3 months, all having GH profile from OGTT. IGF-1 normalization or at least 30% reduction at the last follow-up visit defined a responder patient.
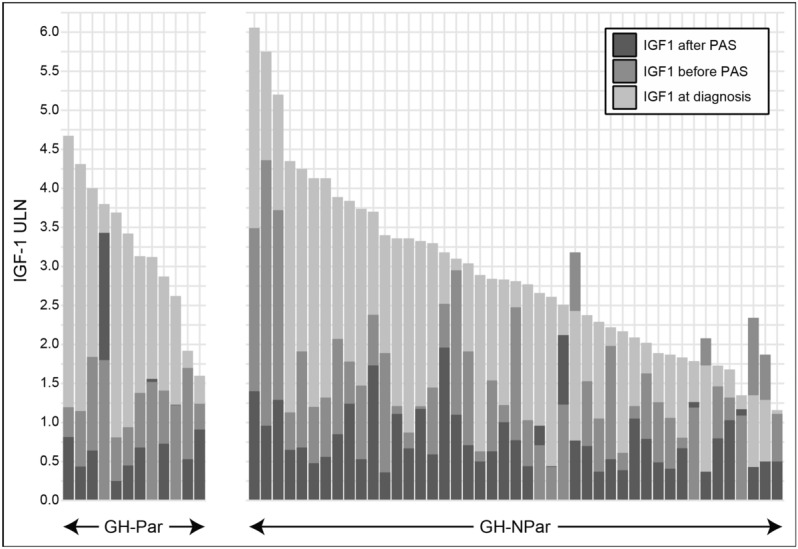
Results: Considering the entire cohort, median IGF-1 levels before pasireotide (available in 57 patients) were 1.38 times the upper limit of normal (ULN) in patients with large (median size 18 mm) and invasive (82%) adenomas after failure of fg-SRL treatment. After a 40-month median treatment, pasireotide effectively reduced IGF-1 ULN levels in 41 patients, 37 of whom achieving normalization, and 4 with a ≥ 30% reduction. Thirteen patients were classified as GH-Par. The median pasireotide duration, dosage, and efficacy (9/12 responder in the GH-Par group and 32/45 in the GH-NPar) were similar between groups. However, the occurrence of new-onset or worsening glucose metabolism alterations (GMAs) after pasireotide was more frequent in GH-NPar (from 37 to 80%; p < 0.001) compared to GH-Par patients (from 69 to 76%), likely due to the higher prevalence of pre-existing GMAs in the GH-Par group before starting pasireotide (p = 0.038).
Conclusions: The GH-Par does not predict the response to pasireotide in acromegaly but can predict a worse metabolic profile.
Keywords: Acromegaly; GH profile; Glucose metabolism alterations; Oral glucose tolerance test; Pasireotide.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: Filippo Ceccato: PhD grant by Novartis Pharma. Pietro Maffei: consultancy fees or Principal Investigator by Recordati, Pfizer, Camurus. Diego Ferone: honoraria for lectures or advisory boards from Recordati, Ipsen, Novartis-AAA, as well as research grants from Camurus and Pfizer. Federico Gatto: honoraria for lectures, manuscript writing, educational events, and consultancy from Pfizer and Recordati. All other authors declare that they have no conflicts of interest that might be perceived as influencing the impartiality of the reported research.
Figures

Similar articles
-
Pasireotide LAR maintains inhibition of GH and IGF-1 in patients with acromegaly for up to 25 months: results from the blinded extension phase of a randomized, double-blind, multicenter, Phase III study.Pituitary. 2015 Jun;18(3):385-94. doi: 10.1007/s11102-014-0585-6. Pituitary. 2015. PMID: 25103549 Free PMC article. Clinical Trial.
-
Paradoxical GH Increase During OGTT Is Associated With First-Generation Somatostatin Analog Responsiveness in Acromegaly.J Clin Endocrinol Metab. 2019 Mar 1;104(3):856-862. doi: 10.1210/jc.2018-01360. J Clin Endocrinol Metab. 2019. PMID: 30285115
-
Switching patients with acromegaly from octreotide to pasireotide improves biochemical control: crossover extension to a randomized, double-blind, Phase III study.BMC Endocr Disord. 2016 Apr 2;16:16. doi: 10.1186/s12902-016-0096-8. BMC Endocr Disord. 2016. PMID: 27039081 Free PMC article. Clinical Trial.
-
Pasireotide in the Personalized Treatment of Acromegaly.Front Endocrinol (Lausanne). 2021 Mar 16;12:648411. doi: 10.3389/fendo.2021.648411. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 33796079 Free PMC article. Review.
-
Cardiometabolic Risk in Acromegaly: A Review With a Focus on Pasireotide.Front Endocrinol (Lausanne). 2020 Feb 6;11:28. doi: 10.3389/fendo.2020.00028. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 32117056 Free PMC article. Review.
References
-
- Bollerslev J, Heck A, Olarescu NC (2019) MANAGEMENT OF ENDOCRINE DISEASE: Individualised management of acromegaly. Eur J Endocrinol 181(2):R57–R71. 10.1530/EJE-19-0124 - PubMed
-
- Muhammad A, Coopmans EC, Gatto F, Franck SE, Janssen JAMJL, van der Lely AJ, Hofland LJ, Neggers SJCMM (2018) Pasireotide responsiveness in acromegaly is mainly driven by somatostatin receptor subtype 2 expression. J Clin Endocrinol Metab. 10.1210/jc.2018-01524 - PubMed
-
- Chiloiro S, Bianchi A, Giampietro A, Pontecorvi A, Raverot G, De Marinis L (2022) Second line treatment of acromegaly: Pasireotide or Pegvisomant? Best Pract Res Clin Endocrinol Metab 36(6):101684. 10.1016/J.BEEM.2022.101684 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
