

Sex Differences in Long COVID
- PMID: 39841477
- PMCID: PMC11755195
- DOI: 10.1001/jamanetworkopen.2024.55430
Sex Differences in Long COVID
Erratum in
-
Errors in Supplement 2.JAMA Netw Open. 2025 Mar 3;8(3):e254888. doi: 10.1001/jamanetworkopen.2025.4888. JAMA Netw Open. 2025. PMID: 40080028 Free PMC article. No abstract available.
Abstract
Importance: A substantial number of individuals worldwide experience long COVID, or post-COVID condition. Other postviral and autoimmune conditions have a female predominance, but whether the same is true for long COVID, especially within different subgroups, is uncertain.
Objective: To evaluate sex differences in the risk of developing long COVID among adults with SARS-CoV-2 infection.
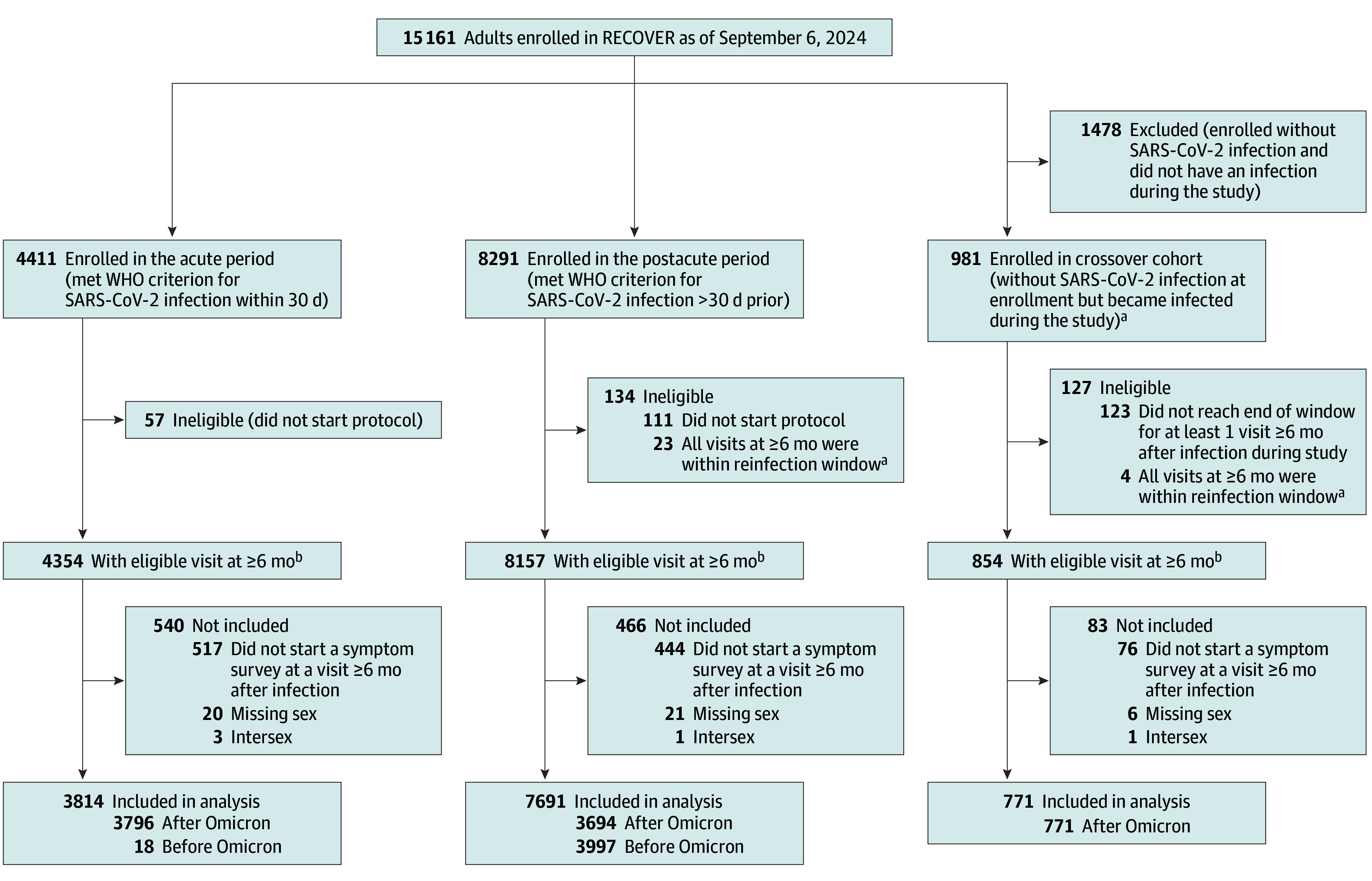
Design, setting, and participants: This cohort study used data from the National Institutes of Health (NIH) Researching COVID to Enhance Recovery (RECOVER)-Adult cohort, which consists of individuals enrolled in and prospectively followed up at 83 sites in 33 US states plus Washington, DC, and Puerto Rico. Data were examined from all participants enrolled between October 29, 2021, and July 5, 2024, who had a qualifying study visit 6 months or more after their initial SARS-CoV-2 infection.
Exposure: Self-reported sex (male, female) assigned at birth.
Main outcomes and measures: Development of long COVID, measured using a self-reported symptom-based questionnaire and scoring guideline at the first study visit that occurred at least 6 months after infection. Propensity score matching was used to estimate risk ratios (RRs) and risk differences (95% CIs). The full model included demographic and clinical characteristics and social determinants of health, and the reduced model included only age, race, and ethnicity.
Results: Among 12 276 participants who had experienced SARS-CoV-2 infection (8969 [73%] female; mean [SD] age at infection, 46 [15] years), female sex was associated with higher risk of long COVID in the primary full (RR, 1.31; 95% CI, 1.06-1.62) and reduced (RR, 1.44; 95% CI, 1.17-1.77) models. This finding was observed across all age groups except 18 to 39 years (RR, 1.04; 95% CI, 0.72-1.49). Female sex was associated with significantly higher overall long COVID risk when the analysis was restricted to nonpregnant participants (RR, 1.50; 95%: CI, 1.27-1.77). Among participants aged 40 to 54 years, the risk ratio was 1.42 (95% CI, 0.99-2.03) in menopausal female participants and 1.45 (95% CI, 1.15-1.83) in nonmenopausal female participants compared with male participants.
Conclusions and relevance: In this prospective cohort study of the NIH RECOVER-Adult cohort, female sex was associated with an increased risk of long COVID compared with male sex, and this association was age, pregnancy, and menopausal status dependent. These findings highlight the need to identify biological mechanisms contributing to sex specificity to facilitate risk stratification, targeted drug development, and improved management of long COVID.
Conflict of interest statement
Figures
References
-
- World Health Organization. WHO COVID-19 dashboard. Accessed September 14, 2024. https://covid19.who.int/region/amro/country/us
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
