

Ten Machine Learning Models for Predicting Preoperative and Postoperative Coagulopathy in Patients With Trauma: Multicenter Cohort Study
- PMID: 39841523
- PMCID: PMC11799815
- DOI: 10.2196/66612
Ten Machine Learning Models for Predicting Preoperative and Postoperative Coagulopathy in Patients With Trauma: Multicenter Cohort Study
Abstract
Background: Recent research has revealed the potential value of machine learning (ML) models in improving prognostic prediction for patients with trauma. ML can enhance predictions and identify which factors contribute the most to posttraumatic mortality. However, no studies have explored the risk factors, complications, and risk prediction of preoperative and postoperative traumatic coagulopathy (PPTIC) in patients with trauma.
Objective: This study aims to help clinicians implement timely and appropriate interventions to reduce the incidence of PPTIC and related complications, thereby lowering in-hospital mortality and disability rates for patients with trauma.
Methods: We analyzed data from 13,235 patients with trauma from 4 medical centers, including medical histories, laboratory results, and hospitalization complications. We developed 10 ML models in Python (Python Software Foundation) to predict PPTIC based on preoperative indicators. Data from 10,023 Medical Information Mart for Intensive Care patients were divided into training (70%) and test (30%) sets, with 3212 patients from 3 other centers used for external validation. Model performance was assessed with 5-fold cross-validation, bootstrapping, Brier score, and Shapley additive explanation values.
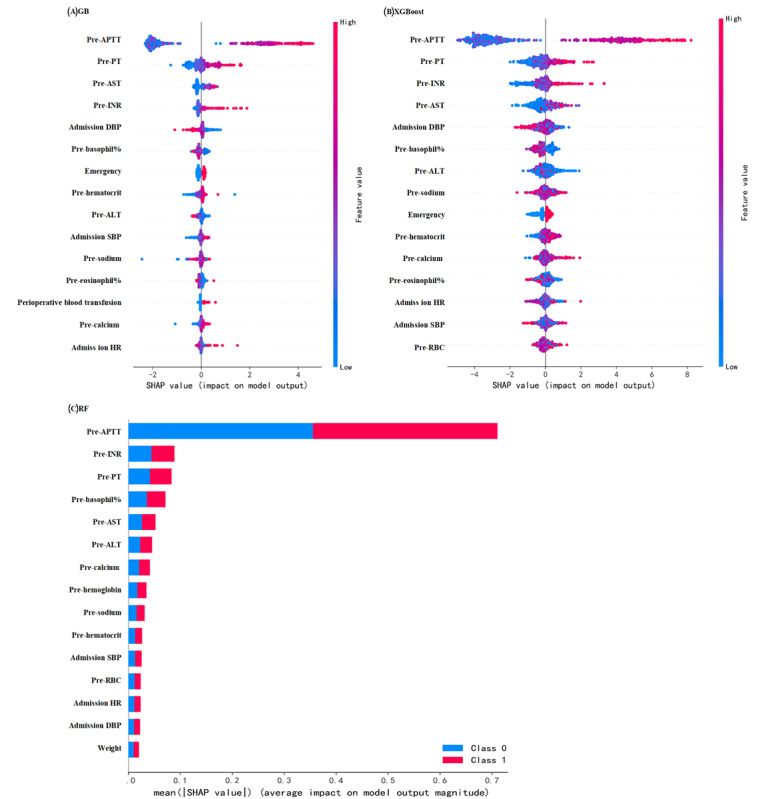
Results: Univariate logistic regression identified PPTIC risk factors as (1) prolonged activated partial thromboplastin time, prothrombin time, and international normalized ratio; (2) decreased levels of hemoglobin, hematocrit, red blood cells, calcium, and sodium; (3) lower admission diastolic blood pressure; (4) elevated alanine aminotransferase and aspartate aminotransferase levels; (5) admission heart rate; and (6) emergency surgery and perioperative transfusion. Multivariate logistic regression revealed that patients with PPTIC faced significantly higher risks of sepsis (1.75-fold), heart failure (1.5-fold), delirium (3.08-fold), abnormal coagulation (3.57-fold), tracheostomy (2.76-fold), mortality (2.19-fold), and urinary tract infection (1.95-fold), along with longer hospital and intensive care unit stays. Random forest was the most effective ML model for predicting PPTIC, achieving an area under the receiver operating characteristic of 0.91, an area under the precision-recall curve of 0.89, accuracy of 0.84, sensitivity of 0.80, specificity of 0.88, precision of 0.88, F1-score of 0.84, and Brier score of 0.13 in external validation.
Conclusions: Key PPTIC risk factors include (1) prolonged activated partial thromboplastin time, prothrombin time, and international normalized ratio; (2) low levels of hemoglobin, hematocrit, red blood cells, calcium, and sodium; (3) low diastolic blood pressure; (4) elevated alanine aminotransferase and aspartate aminotransferase levels; (5) admission heart rate; and (6) the need for emergency surgery and transfusion. PPTIC is associated with severe complications and extended hospital stays. Among the ML models, the random forest model was the most effective predictor.
Trial registration: Chinese Clinical Trial Registry ChiCTR2300078097; https://www.chictr.org.cn/showproj.html?proj=211051.
Keywords: Medical Information Mart for Intensive Care; machine learning models; postoperative; preoperative; random forest; traumatic coagulopathy.
©Xiaojuan Xiong, Hong Fu, Bo Xu, Wang Wei, Mi Zhou, Peng Hu, Yunqin Ren, Qingxiang Mao. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 22.01.2025.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures




Similar articles
-
Supervised Machine Learning Models for Predicting Sepsis-Associated Liver Injury in Patients With Sepsis: Development and Validation Study Based on a Multicenter Cohort Study.J Med Internet Res. 2025 May 26;27:e66733. doi: 10.2196/66733. J Med Internet Res. 2025. PMID: 40418571 Free PMC article.
-
Predicting postoperative trauma-induced coagulopathy in patients with severe injuries by machine learning.Sci Rep. 2025 Jul 25;15(1):27072. doi: 10.1038/s41598-025-13283-x. Sci Rep. 2025. PMID: 40715561 Free PMC article.
-
Development and validation of a machine learning-based model for predicting intraoperative blood loss during burn surgery.Surgery. 2025 Aug;184:109445. doi: 10.1016/j.surg.2025.109445. Epub 2025 May 29. Surgery. 2025. PMID: 40446607
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
References
-
- GBD 2017 Causes of Death Collaborators Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788. doi: 10.1016/S0140-6736(18)32203-7. https://linkinghub.elsevier.com/retrieve/pii/S0140-6736(18)32203-7 S0140-6736(18)32203-7 - DOI - PMC - PubMed
-
- Kornblith LZ, Moore HB, Cohen MJ. Trauma-induced coagulopathy: the past, present, and future. J Thromb Haemost. 2019;17(6):852–862. doi: 10.1111/jth.14450. https://linkinghub.elsevier.com/retrieve/pii/S1538-7836(22)04449-X S1538-7836(22)04449-X - DOI - PMC - PubMed
-
- Maegele M, Lefering R, Yucel N, Tjardes T, Rixen D, Paffrath T, Simanski C, Neugebauer E, Bouillon B. Early coagulopathy in multiple injury: an analysis from the German Trauma Registry on 8724 patients. Injury. 2007;38(3):298–304. doi: 10.1016/j.injury.2006.10.003.S0020-1383(06)00613-9 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
