

Retrospective cross-sectional study on bronchiectasis in adult Aboriginal Australians: disease characteristics and comparison with ethnically diverse global bronchiectasis registry cohorts
- PMID: 39842857
- PMCID: PMC11784196
- DOI: 10.1136/bmjresp-2023-002139
Retrospective cross-sectional study on bronchiectasis in adult Aboriginal Australians: disease characteristics and comparison with ethnically diverse global bronchiectasis registry cohorts
Abstract
Background: Globally, adult Indigenous people, including Aboriginal Australians, have a high burden of chronic respiratory disorders, and bronchiectasis is no exception. However, literature detailing bronchiectasis disease characteristics among adult Indigenous people is sparse. This study assessed the clinical profile of bronchiectasis among adult Aboriginal Australians and compared against previously published international bronchiectasis registry reports.
Methods: Aboriginal Australians aged >18 years with chest CT confirmed bronchiectasis between 2011 and 2020 in the Top End Northern Territory of Australia were included. Demographics, chest CT findings, pulmonary function results, sputum microbiology, coexistent medical comorbidities, and pharmacotherapy use were assessed and compared against five published international bronchiectasis registry reports (Australian (ABR), European (European Multicentre Bronchiectasis Audit and Research Collaboration (EMBARC)-Europe), Indian (EMBARC-India), Korean (KMBARC) and the USA (USBRR)).
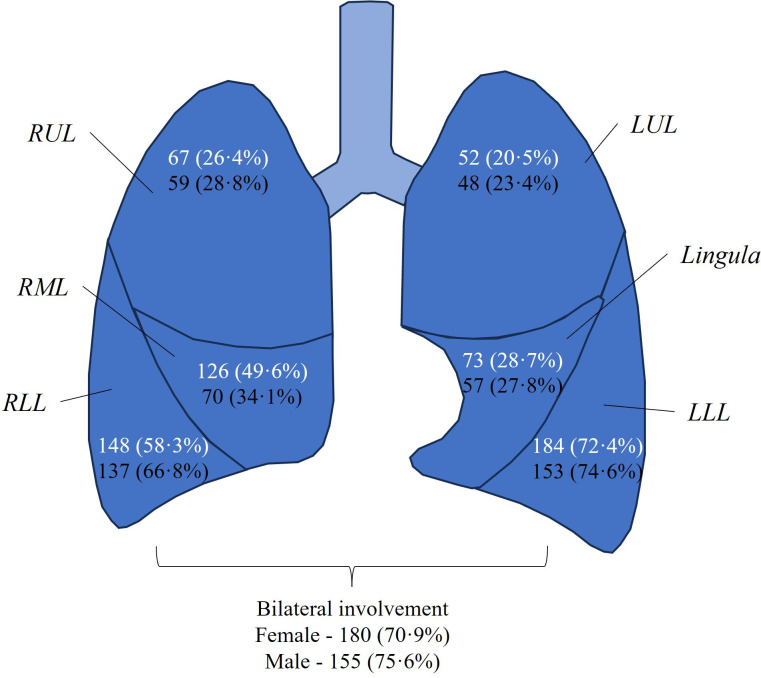
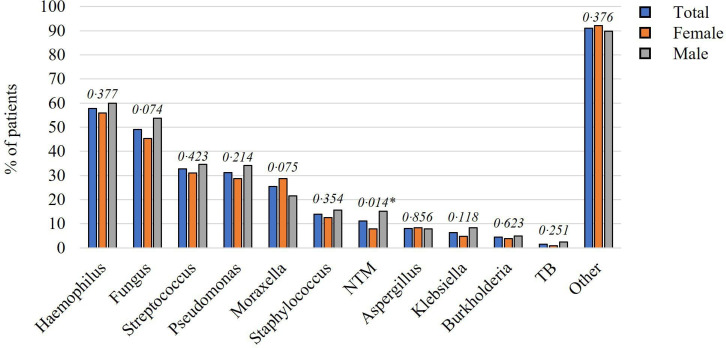
Results: A total of 459 patients were assessed. In comparison with international and non-Aboriginal Australian national cohorts, Aboriginal Australians were younger (median 56 years (IQR (48, 65)); however, sex distribution (55% female) and body mass index (23 kg/m2 (IQR 19.4-27)) were comparable . Smoking rates were higher at 85% compared with other registry cohorts (22-46%) as was the prevalence of comorbidities (97%): cardiovascular diseases (73%), diabetes mellitus (50%) and chronic obstructive pulmonary disease (83%) compared with other registry cohorts (4-32%; 6-14%; and 14-37%, respectively). Spirometry demonstrated forced expiratory volume in 1 s of 38% predicted in comparison with 61-77% in other cohorts. Sputum microbiology showed Haemophilus influenzae (57%) isolated at 3.4 to 6 times the rate of other registry cohorts and Pseudomonas aeruginosa in 31%. Chest CT demonstrated multilobar and lower lobes involvement in 73% and inhaled pharmacotherapy use was recorded in up to 62% and long-term antibiotics in 5%.
Conclusion: The overall bronchiectasis disease burden is higher in Aboriginal Australian adults in comparison with global ethnically diverse non-Indigenous populations. Further efforts are required to address this disparity secondary to bronchiectasis among Indigenous people.
Keywords: Atypical Mycobacterial Infection; Bronchiectasis; COPD epidemiology; Clinical Epidemiology; Emphysema; Imaging/CT MRI etc; Inhaler devices; Respiratory Function Test.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- Howarth T, Heraganahally SS, Heraganahally SS. Bronchiectasis Among Adult First Nations Indigenous People - A Scoping Review. CRMR. 2023;19:36–51. doi: 10.2174/1573398X19666221212164215. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources