

Prognostic role of con-/discordant coronary flow reserve and microvascular resistance in coronary microvascular disease: a systematic review and network meta-analysis
- PMID: 39842937
- PMCID: PMC11759884
- DOI: 10.1136/openhrt-2024-003055
Prognostic role of con-/discordant coronary flow reserve and microvascular resistance in coronary microvascular disease: a systematic review and network meta-analysis
Abstract
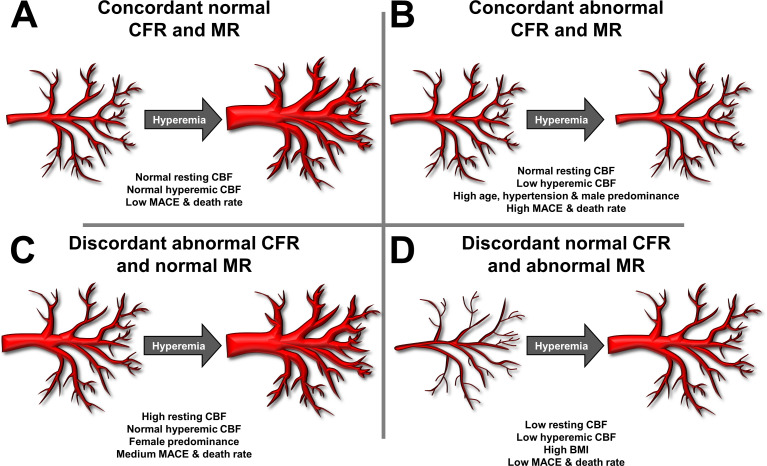
Background: Coronary microvascular disease (CMD) is defined as impaired coronary flow reserve (CFR) and/or increased microvascular resistance (MR) without significant epicardial coronary stenosis. This definition allows for discordant CFR and MR values within patients with CMD. The aim of this meta-analysis is to characterise the prognostic value and pathophysiological backgrounds of CFR and MR con-/discordance.
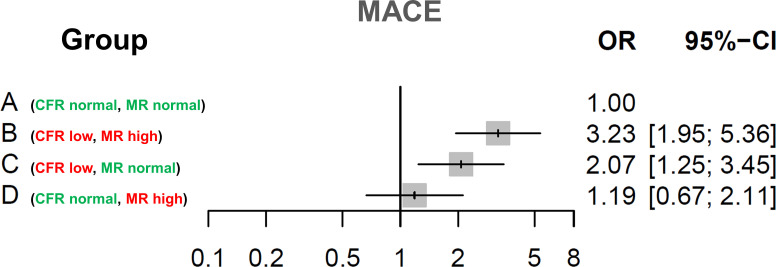
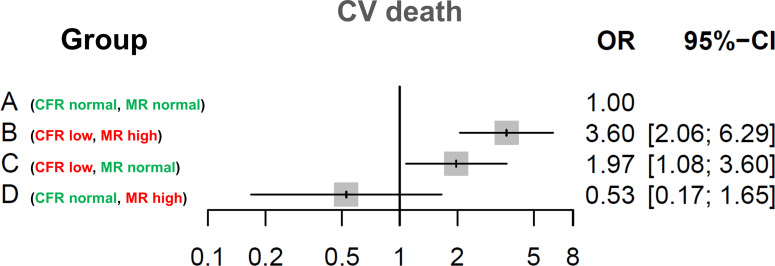
Methods: A systematic search (PROSPERO CRD42024573004) identified studies determining CFR and MR in patients without significant epicardial coronary artery disease. Patients were divided into four groups: (1) normal CFR and MR, (2) abnormal CFR and MR, (3) abnormal CFR with normal MR and (4) normal CFR with abnormal MR and analysed for all-cause mortality and major adverse cardiovascular events (MACE).
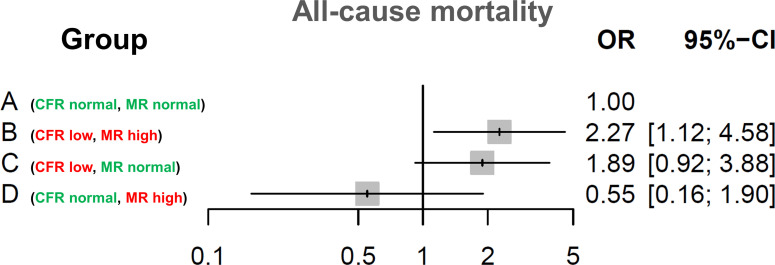
Results: We identified four studies representing 2310 total participants. Group B had the highest MACE (OR: 3.23; 95% CI 1.95 to 5.36) and mortality rate (OR: 2.27; 95% CI 1.12 to 4.58) compared with group A. Group C, associated with female sex, showed significantly higher MACE (OR: 2.07; 95% CI 1.25 to 3.45) but not mortality (OR: 1.89; 95% CI 0.92 to 3.88) compared with group A. In group D, associated with high body mass index, MACE and mortality rates did not differ significantly from group A (OR: 1.19; 95% CI 0.67 to 2.11 and OR: 0.55; 95% CI 0.16 to 1.90, respectively).
Conclusions: Abnormal CFR and MR are associated with a high risk of MACE and death. Abnormal CFR and normal MR are associated with an increased MACE-but not death. MACE and mortality risk in discordantly normal CFR and abnormal MR are low. Our findings show the need for tailoring CFR and MR diagnostic thresholds to patient characteristics and raise questions about the presence of CMD in patients with abnormal MR with normal CFR.
Keywords: Angina Pectoris; Chest Pain; Coronary Angiography; Meta-Analysis; Microvascular Angina.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: The Department of Cardiology of the Leiden University Medical Center received unrestricted research grants from Abbott Vascular, Bayer, Biotronik, Boston Scientific, Edwards Lifesciences, GE Healthcare and Medtronic. JMM-C received a research grant from Shockwave Medical and Speaker fees from Penumbra, Abiomed and Boston Scientific.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical