

Temporal order of atrial fibrillation and acute myocardial infarction and associated prognosis in the Danish Diet, Cancer and Health cohort
- PMID: 39842938
- PMCID: PMC11759883
- DOI: 10.1136/openhrt-2024-003132
Temporal order of atrial fibrillation and acute myocardial infarction and associated prognosis in the Danish Diet, Cancer and Health cohort
Abstract
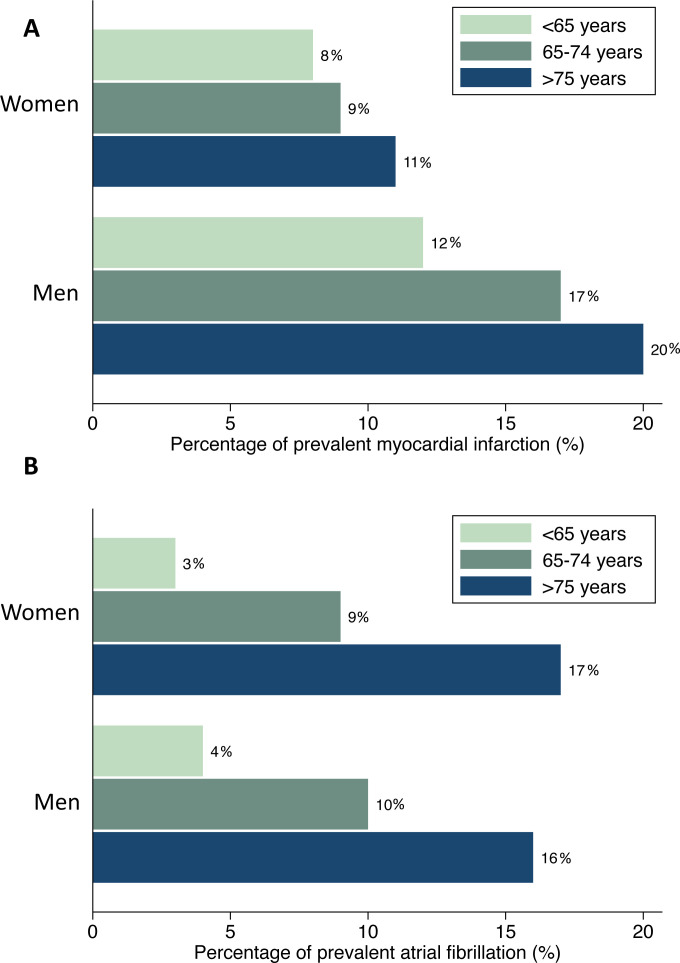
Background: Atrial fibrillation (AF) and acute myocardial infarction (AMI) share risk factors and are bidirectionally associated. Several studies found higher risks of outcomes in individuals with both conditions. Whether the risks of outcomes differ according to temporal order of AF and AMI is unclear.
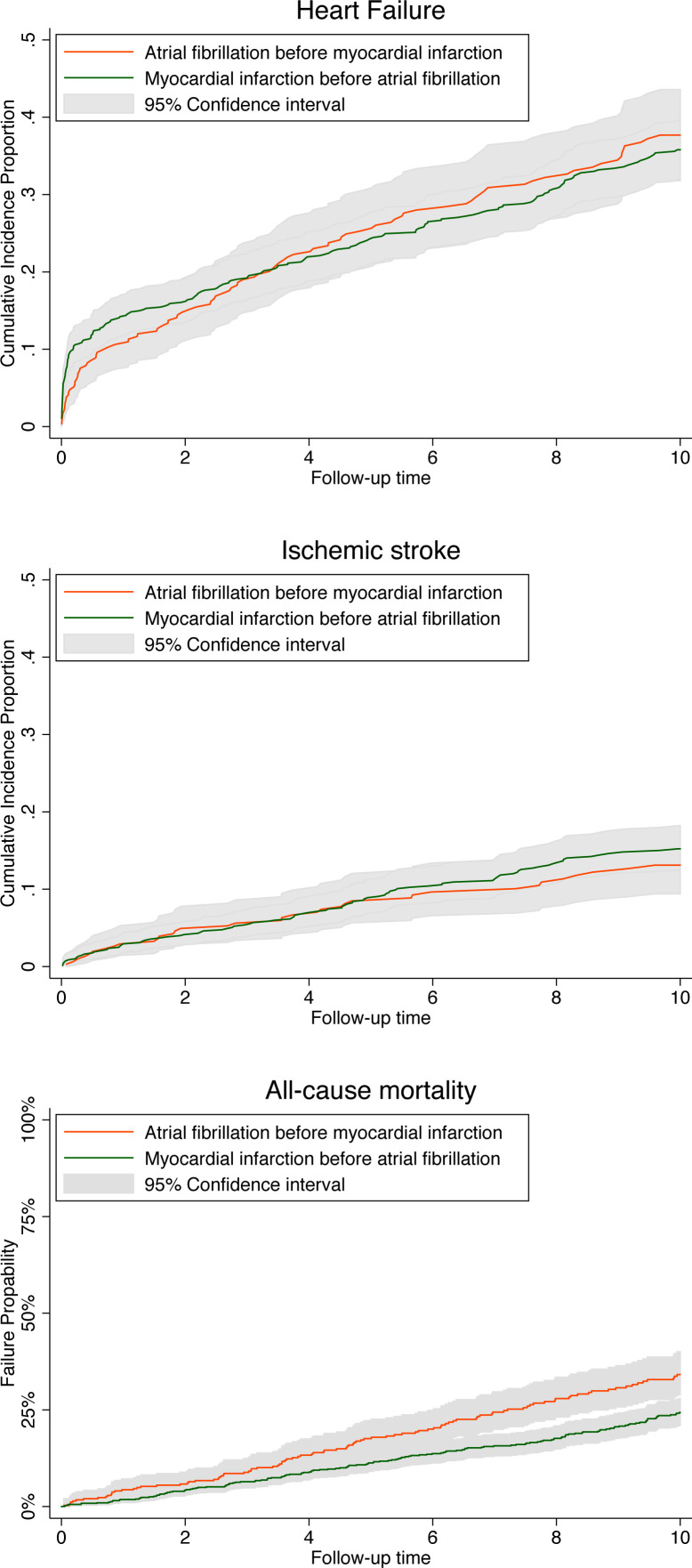
Methods: The study was based on the Danish Diet, Cancer and Health cohort. We assessed the risk of heart failure (HF), ischaemic stroke (IS) and all-cause mortality during 10 years of follow-up in participants with both AF and AMI compared with only one and according to the temporal order of AF and AMI in participants with both conditions.
Results: We identified 5816 participants with newly diagnosed AF only, 3448 with first AMI only, 348 with AF before AMI and 721 participants with AMI before AF. The multivariable-adjusted risks of HF, IS and all-cause mortality were higher among participants with both AF and AMI compared with participants with only AF or AMI. In participants with both, there was no difference in risk of HF (HR 0.92, 95% CI 0.72 to 1.17) or IS (HR 1.12, 95% CI 0.76 to 1.66) between participants with AF before AMI compared with AMI before AF. AMI before AF was associated with lower all-cause mortality compared with AF before AMI (HR 0.70, 95% CI 0.54 to 0.90).
Conclusions: Risks of adverse outcomes were higher among participants with both AF and AMI compared with only AF or AMI. All-cause mortality, but not risk of HF or IS, differed according to temporal order with a lower mortality among participants with AMI before AF.
Keywords: Acute Coronary Syndrome; Atrial Fibrillation; Epidemiology; Risk Factors.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: HKJ received lecture fees from Abbott Denmark and Biosense Webster, Europe. There are no other conflicts of interest to declare.
Figures
Similar articles
-
Association of Atrial Fibrillation Burden With Cardiovascular Outcomes in New-Onset Atrial Fibrillation Complicating Myocardial Infarction.J Am Heart Assoc. 2025 May 20;14(10):e039547. doi: 10.1161/JAHA.124.039547. Epub 2025 Apr 16. J Am Heart Assoc. 2025. PMID: 40240944 Free PMC article.
-
Prognosis of patients with acute myocardial infarction in the setting of COVID-19: A French nationwide observational study.Arch Cardiovasc Dis. 2025 May;118(5):312-321. doi: 10.1016/j.acvd.2025.01.008. Epub 2025 Mar 18. Arch Cardiovasc Dis. 2025. PMID: 40157843
-
Atrial fibrillation and the risk for myocardial infarction, all-cause mortality and heart failure: A systematic review and meta-analysis.Eur J Prev Cardiol. 2017 Sep;24(14):1555-1566. doi: 10.1177/2047487317715769. Epub 2017 Jun 15. Eur J Prev Cardiol. 2017. PMID: 28617620 Free PMC article.
-
Remote ischaemic preconditioning for coronary artery bypass grafting (with or without valve surgery).Cochrane Database Syst Rev. 2017 May 5;5(5):CD011719. doi: 10.1002/14651858.CD011719.pub3. Cochrane Database Syst Rev. 2017. PMID: 28475274 Free PMC article.
-
Beta-blockers in patients without heart failure after myocardial infarction.Cochrane Database Syst Rev. 2021 Nov 5;11(11):CD012565. doi: 10.1002/14651858.CD012565.pub2. Cochrane Database Syst Rev. 2021. PMID: 34739733 Free PMC article.
References
-
- Luo C-F, Mo P, Li G-Q, et al. Aspirin-omitted dual antithrombotic therapy in non-valvular atrial fibrillation patients presenting with acute coronary syndrome or undergoing percutaneous coronary intervention: results of a meta-analysis. Eur Heart J Cardiovasc Pharmacother. 2021;7:218–24. doi: 10.1093/ehjcvp/pvaa016. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous