

A systematic review of emergency room laparotomy in patients with severe abdominal trauma
- PMID: 39843466
- PMCID: PMC11754590
- DOI: 10.1038/s41598-025-87241-y
A systematic review of emergency room laparotomy in patients with severe abdominal trauma
Abstract
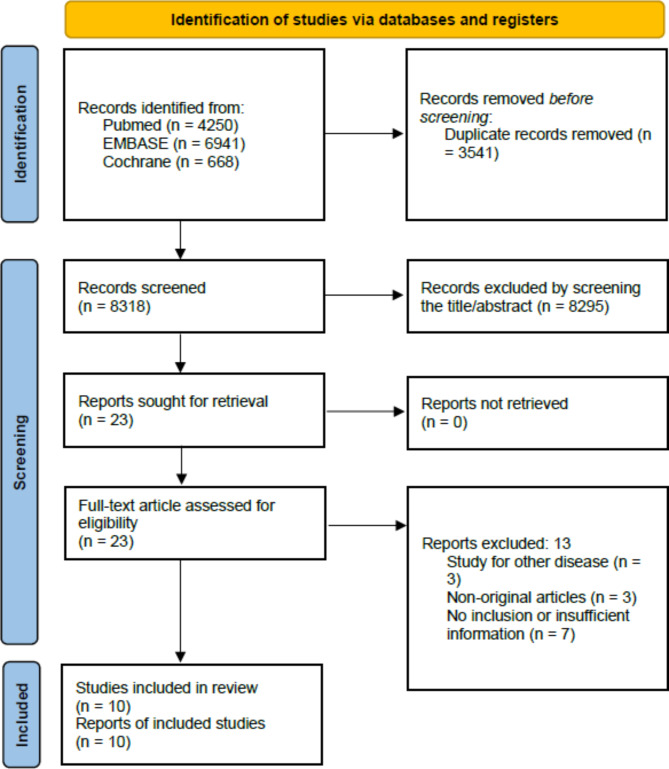
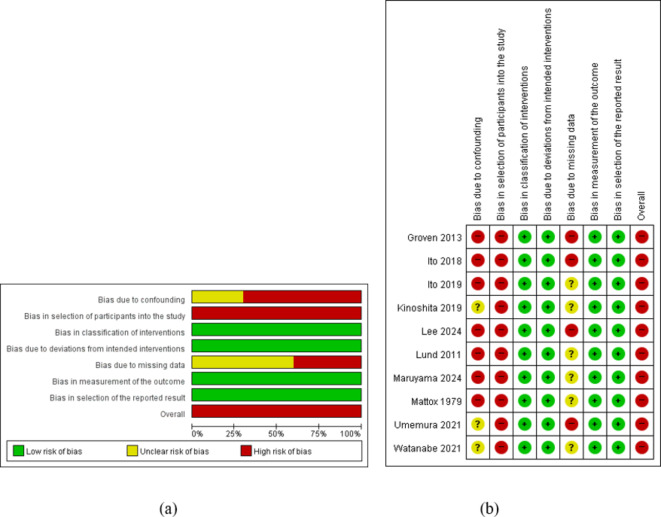
Traumatic intra-abdominal hemorrhage contributes to mortality in patients with trauma. However, initiating an emergent laparotomy in the operating room (OR) as a standard treatment can sometimes be time-consuming. To overcome this issue, laparotomy is performed in the emergency room (ER) in some institutions. This systematic review evaluates the efficacy of performing ER laparotomy. Comprehensive searches were conducted in MEDLINE PubMed, EMBASE, and Cochrane databases, up to August 9, 2024. The risk of bias in observational studies was assessed using the ROBINS-I tool. The primary outcome was mortality following ER laparotomy, and the secondary outcome was time from admission to first laparotomy. The review included 10 studies, all of which were observational. A meta-analysis was not performed due to substantial heterogeneity and insufficient data. Mortality rates after ER laparotomy ranged from 23 to 100%. Mortality rates were 23.0-66.7% in the conventional ER group, while they were 0-30% in the OR group. In the hybrid ER group, the 28-day mortality rates were 12.7-15%, compared to 21.7-22% in the conventional group. The time from admission to the first laparotomy was 17-43 min (median) in the conventional ER group, compared to 40-111 min (median) in the OR laparotomy group. In the hybrid ER setting, the time from admission to intervention, including laparotomy, was 35-48 min (median), whereas it was 72-101 min (median) in the conventional group. A high and unclear risk of bias due to confounding was noted across the studies. ER laparotomy may provide rapid bleeding control. However, due to the limited number of studies and significant heterogeneity among the studies reviewed, the true effect size of ER laparotomy in conventional and hybrid ER settings remains unclear.
Keywords: Abdomen; Emergency room; Hemorrhage; Laparotomy; Systematic review.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
References
-
- Park, Y. et al. Major causes of preventable death in trauma patients. J. Trauma Inj.34, 225–232 (2021). - DOI
-
- Clarke, J. R., Trooskin, S. Z., Doshi, P. J., Greenwald, L. & Mode, C. J. Time to laparotomy for intra-abdominal bleeding from trauma does affect survival for delays up to 90 minutes. J. Trauma52, 420–425 (2002). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
