

Patterns of psychiatric healthcare use during pandemic times among boys and girls with pre-existing diagnoses: a Norwegian nationwide primary and specialist healthcare registry study
- PMID: 39844080
- PMCID: PMC11756222
- DOI: 10.1186/s12888-024-06422-7
Patterns of psychiatric healthcare use during pandemic times among boys and girls with pre-existing diagnoses: a Norwegian nationwide primary and specialist healthcare registry study
Abstract
Background: The COVID-19 pandemic introduced complexities that were likely more demanding for some groups, such as children and adolescents, and especially those with pre-existing mental health diagnoses. This study examines long-term patterns of psychiatric healthcare use among this vulnerable group, providing insights into shifts in psychiatric healthcare use during a global health crisis.
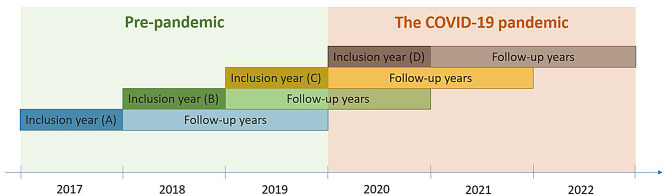
Methods: We use data from the primary and specialist healthcare registries available from the Norwegian emergency preparedness register for COVID-19 (Beredt C19) to estimate patterns of psychiatric healthcare use. The data spans 2017 to 2022, covering children and adolescents aged 6-19. We identified young people with recent diagnoses of mental health conditions and compared weekly consultation volumes before and during the pandemic for mental health conditions overall and the following diagnostic or symptom categories separately: anxiety/depression and Attention-Deficit Hyperactivity Disorders (ADHD). Analyses were stratified by gender.
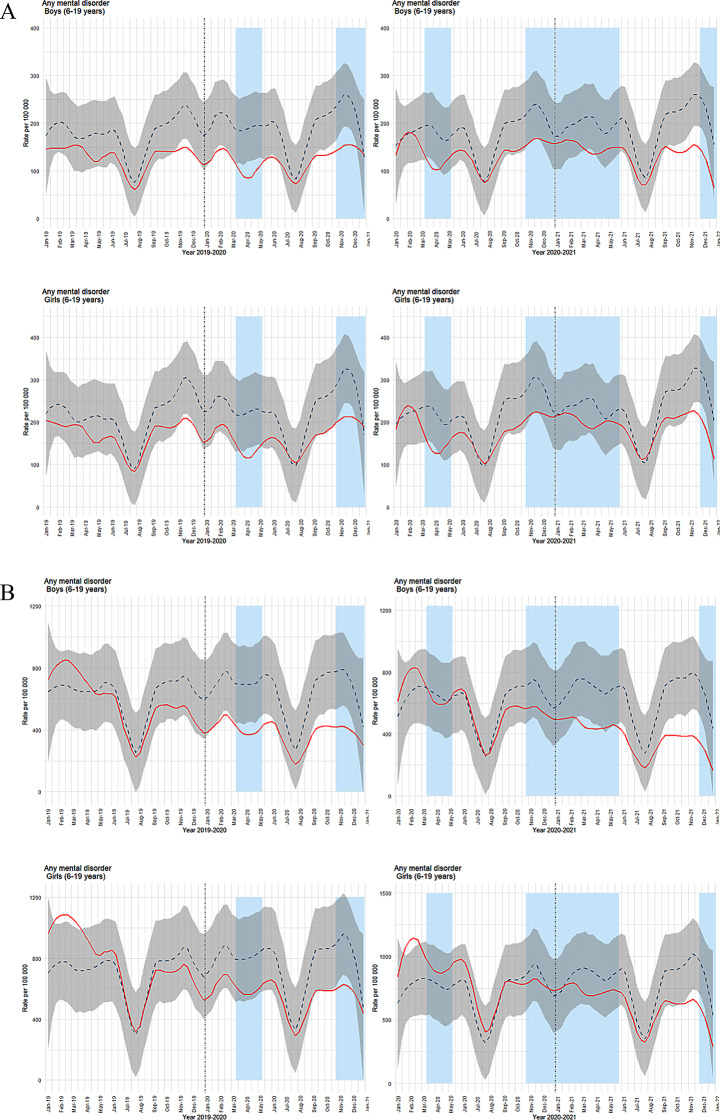
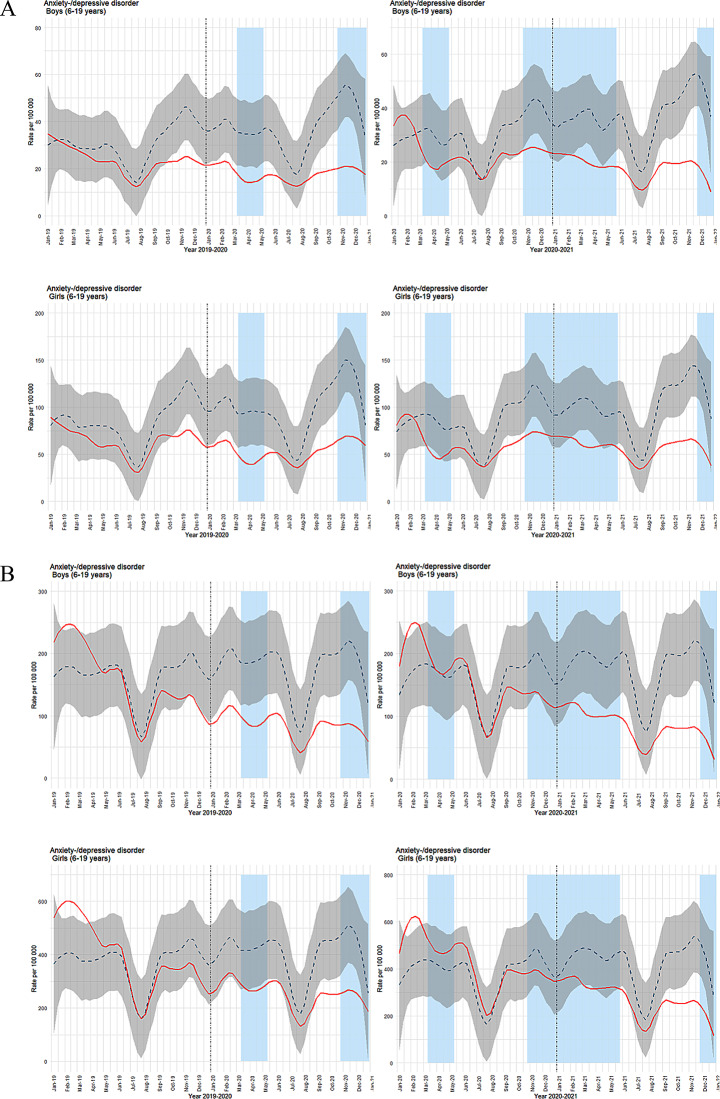
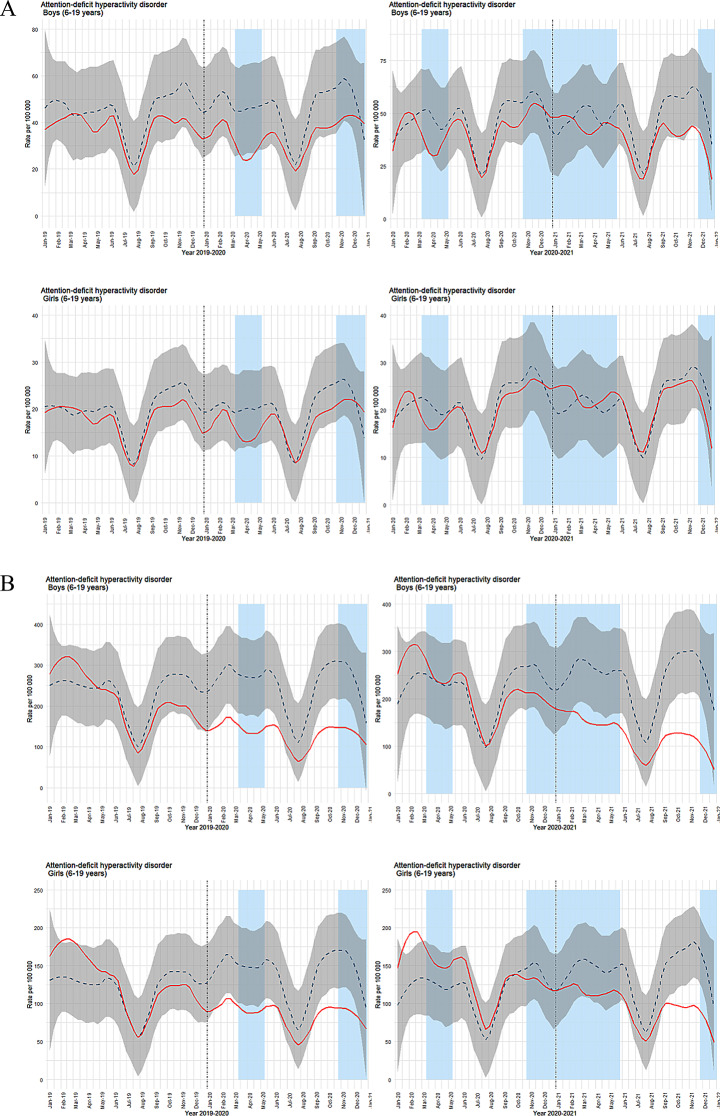
Results: There was a consistent trend of lower-than-predicted weekly healthcare consultations among young people with pre-existing mental health diagnoses in both primary and specialist healthcare during the pandemic. The reduction was more pronounced in later follow-up periods. The study highlights gender disparities, with boys experiencing more notable declines in healthcare consultations, especially in specialist care. Additionally, the time trends varied across different diagnostic groups. While consultations for anxiety/depression were consistently below the predicted levels, declines in ADHD occurred later in the pandemic. The data suggests an overall decline in healthcare use rather than a shift between sectors.
Conclusion: The findings offer insights into healthcare use during pandemic times among children and adolescents with pre-existing mental health diagnoses. The study underscores the importance of continuous monitoring and support for this group, ensuring accessible and responsive healthcare during public health emergencies.
Keywords: Adolescents; COVID-19; Children; Health registry; Mental disorders; Primary health care; Specialist health care; Time trends.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Regional Ethics Committee for Medical Research South-East Norway approved the current study #267200. For data minimization purposes, we only had access to the data needed from the Beredt C19, not the entire database (data minimization). Data was based on de-identified and routinely collected registry data from the Norwegian population. According to the Norwegian Health Registry Act § 19, The Regional Ethics Committee for Medical Research South-East Norway waived the informed consent requirement. The study was carried out following the ethical standards of the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Migrant background and the impact of the COVID-19 pandemic on mental healthcare consultations among children and adolescents in Norway: a nationwide registry study.BMC Health Serv Res. 2023 Jun 30;23(1):718. doi: 10.1186/s12913-023-09666-3. BMC Health Serv Res. 2023. PMID: 37391771 Free PMC article.
-
Patterns and correlates of mental healthcare utilization during the COVID-19 pandemic among individuals with pre-existing mental disorder.PLoS One. 2024 Jun 4;19(6):e0303079. doi: 10.1371/journal.pone.0303079. eCollection 2024. PLoS One. 2024. PMID: 38833458 Free PMC article.
-
Impact of the COVID-19 pandemic on mental healthcare consultations among children and adolescents in Norway: a nationwide registry study.Eur Child Adolesc Psychiatry. 2023 Jun;32(6):1025-1035. doi: 10.1007/s00787-022-02046-y. Epub 2022 Jul 27. Eur Child Adolesc Psychiatry. 2023. PMID: 35896740 Free PMC article.
-
Psychosocial alterations during the COVID-19 pandemic and the global burden of anxiety and major depressive disorders in adolescents, 1990-2021: challenges in mental health amid socioeconomic disparities.World J Pediatr. 2024 Oct;20(10):1003-1016. doi: 10.1007/s12519-024-00837-8. Epub 2024 Aug 20. World J Pediatr. 2024. PMID: 39162949 Review.
-
Service design for children and young people with common mental health problems: literature review, service mapping and collective case study.Health Soc Care Deliv Res. 2024 May;12(13):1-181. doi: 10.3310/DKRT6293. Health Soc Care Deliv Res. 2024. PMID: 38767587 Review.
References
-
- WHO. Mental health and covid-19: scientific brief; 2022.
-
- Nøkleby H, Borge TC, Lidal IB, Bjerke Johansen T, Langøyen LJ. Konsekvenser Av covid-19-pandemien for barn og unges Liv Og psykiske helse: andre oppdatering av en hurtigoversikt [Consequences of the Covid-19 pandemic on children and youth’s life and mental health: second update of a rapid review]. Norway: Oslo; 2023.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
