

Management of children with food allergies by allergists in the United States
- PMID: 39844911
- PMCID: PMC11750536
- DOI: 10.1016/j.jacig.2024.100379
Management of children with food allergies by allergists in the United States
Abstract
Background: Management of patients with food allergies is complex, especially in cases of patients with multiple and potentially severe food allergies. Although international guidelines exist for food allergy management, the role of the allergist in the decision-making process is key.
Objective: Our aim was to investigate the management patterns and educational needs of practicing allergists treating patients with food allergies.
Methods: An online survey was e-mailed to United States-based practicing allergists (N = 2833) in November-December 2021. The allergists were screened for managing 1 or more patients (including ≥25% pediatric patients) with food allergies per month. The allergists responded to questions regarding food allergy management in response to 2 hypothetical pediatric case studies, their familiarity with available guidelines and emerging treatments, and their future educational preferences. A descriptive analysis of outcomes was conducted.
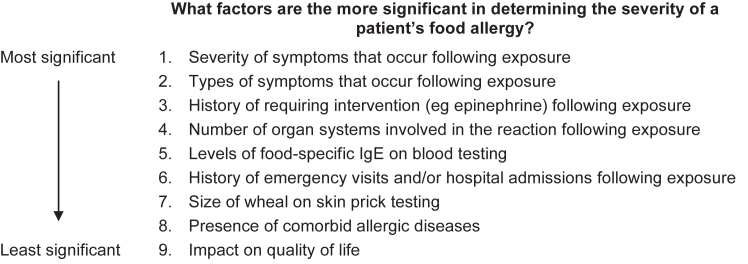
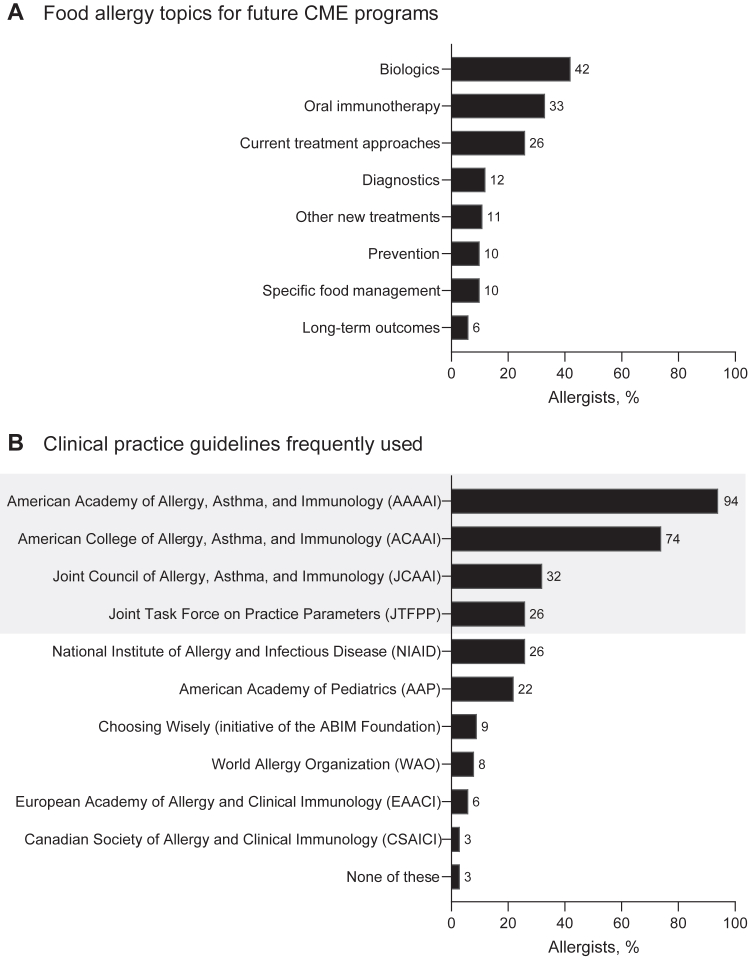
Results: A total of 125 responding allergists (4.4%) met the eligibility criteria and completed the survey. The allergists prioritized written exposure action plans, patient-caregiver communication, prevention of serious reactions, and consideration of both food allergy severity and allergic comorbidities in the management of patients with food allergies. With regard to recommending biologics in the future, the allergists identified patient history of anaphylaxis and hospitalizations, food allergy severity, and allergic comorbidities as all being important factors to consider when deciding on appropriate treatment options. The allergists noted their ongoing educational needs, especially for current and emerging treatments for food allergies.
Conclusion: With the treatment landscape for food allergies evolving rapidly, the decision-making priorities and continuing educational needs of allergists will be important in optimizing the management of patients with food allergies.
Keywords: Allergists; anaphylaxis; children; continuing; education; food allergy; food hypersensitivity; medical; pediatric.
© 2024 The Author(s).
Conflict of interest statement
Conducted by CE Outcomes, LLC, with support from Genentech, Inc, a member of the Roche Group. Disclosure of potential conflicts of interest: A. Anagnostou reports receiving institutional funding from Aimmune, Mike Hogg Foundation and Novartis; serving as an advisory board member for DBV Technologies and Novartis; receiving consultation and/or speaker fees from Adelphi, Aimmune, ALK, and Genentech, Inc. M. Greenhawt reports being a consultant for Aquestive; serving as an advisory board member for Aquestive, ALK-Abelló, Allergy Therapeutics, AstraZeneca, Bryn Pharma, DBV Technologies, Novartis, Nutricia, and Prota; serving as an unpaid member of the scientific advisory council for the National Peanut Board; sitting on the medical advisory board of the International Food Protein–Induced Enterocolitis Syndrome Association; serving as a member of the Brighton Collaboration Criteria Vaccine Anaphylaxis 2.0 working group; acting as senior associate editor for the Annals of Allergy, Asthma, and Immunology; and serving as a member of the Joint Task Force on Allergy Practice Parameters. J. A. Lieberman reports serving as an advisory board member for Aquestive; sitting on the data and safety and monitoring board and/or adjudication committee for AbbVie and Siolta; acting as a consultant for ALK, Bayer, DBV, and Novartis; and serving as a board member for the American Board of Allergy and Immunology and Joint Task Force for Practice Parameters. C. E. Ciaccio reports providing research support from the Duchossois Foundation, Food Allergy Research and Education (FARE), National Institutes of Health, and Paul and Mary Yovovich; and serving as an advisory board member for Clostrabio, Genentech, Inc, and Siolta. S. B. Sindher reports receiving grants from Aimmune, Consortium for Food Allergy Research (CoFAR), DBV, the National Institute for Allergy and Infectious Diseases (NIAID), Novartis, Regeneron, and Sanofi and serving as an advisory board member for Genentech, Inc. B. Creasy, K. Baran, and S. Gupta are employees of Genentech, Inc, and stockholders in Roche. A. Nowak-Wegrzyn reports receiving research support from Astellas, Danone, DBV, the NIAID, and Nestlé; receiving consultancy fees from Gerber Institute, Novartis, and Regeneron; acting as deputy editor for Annals of Allergy, Asthma, and Immunology; and serving as chair of the medical advisory board of the International Food Protein–Induced Enterocolitis Syndrome Association.
Figures



Similar articles
-
Food Oral Immunotherapy: A Survey Among US Practicing Allergists Conducted as a AAAAI Leadership Institute Project and Work Group Report.J Allergy Clin Immunol Pract. 2023 Aug;11(8):2330-2334. doi: 10.1016/j.jaip.2023.03.060. Epub 2023 May 24. J Allergy Clin Immunol Pract. 2023. PMID: 37236350
-
Food allergy management from the perspective of patients or caregivers, and allergists: a qualitative study.Allergy Asthma Clin Immunol. 2010 Nov 30;6(1):30. doi: 10.1186/1710-1492-6-30. Allergy Asthma Clin Immunol. 2010. PMID: 21118534 Free PMC article.
-
A study to assess current approaches of allergists in European countries diagnosing and managing children and adolescents with peanut allergy.PLoS One. 2020 Dec 3;15(12):e0241648. doi: 10.1371/journal.pone.0241648. eCollection 2020. PLoS One. 2020. PMID: 33270629 Free PMC article.
-
Management of food allergies in schools: a perspective for allergists.J Allergy Clin Immunol. 2009 Aug;124(2):175-82, 182.e1-4; quiz 183-4. doi: 10.1016/j.jaci.2009.04.004. Epub 2009 Jun 3. J Allergy Clin Immunol. 2009. PMID: 19493563 Review.
-
Primary prevention of food allergy in 2021: Update and proposals of French-speaking pediatric allergists.Arch Pediatr. 2022 Feb;29(2):81-89. doi: 10.1016/j.arcped.2021.11.009. Epub 2021 Dec 23. Arch Pediatr. 2022. PMID: 34955309 Review.
Cited by
-
US food allergy patients' experiences, priorities, and needs: A qualitative study.J Allergy Clin Immunol Glob. 2025 Apr 22;4(3):100482. doi: 10.1016/j.jacig.2025.100482. eCollection 2025 Aug. J Allergy Clin Immunol Glob. 2025. PMID: 40486694 Free PMC article.
-
Trade-offs from a family perspective: considerations in choosing between omalizumab and complementary alternative medicine for pediatric severe asthma.Front Pharmacol. 2025 Jul 31;16:1621101. doi: 10.3389/fphar.2025.1621101. eCollection 2025. Front Pharmacol. 2025. PMID: 40822491 Free PMC article. Review.
References
-
- Wang J., Sampson H.A., Fiocchi A., Sicherer S., WAO . In: Asthma: comorbidities, coexisting conditions, and differential diagnosis. Lockey R.F., Ledford D.K., editors. Oxford University Press; Oxford, UK: 2014. Atopic dermatitis, food allergy, and anaphylaxis: comorbid and coexisting; pp. 455–466.
LinkOut - more resources
Full Text Sources
Miscellaneous
