

Weather and prehospital predictors of trauma patient mortality in a rural American state
- PMID: 39845067
- PMCID: PMC11749964
- DOI: 10.1016/j.sipas.2022.100066
Weather and prehospital predictors of trauma patient mortality in a rural American state
Abstract
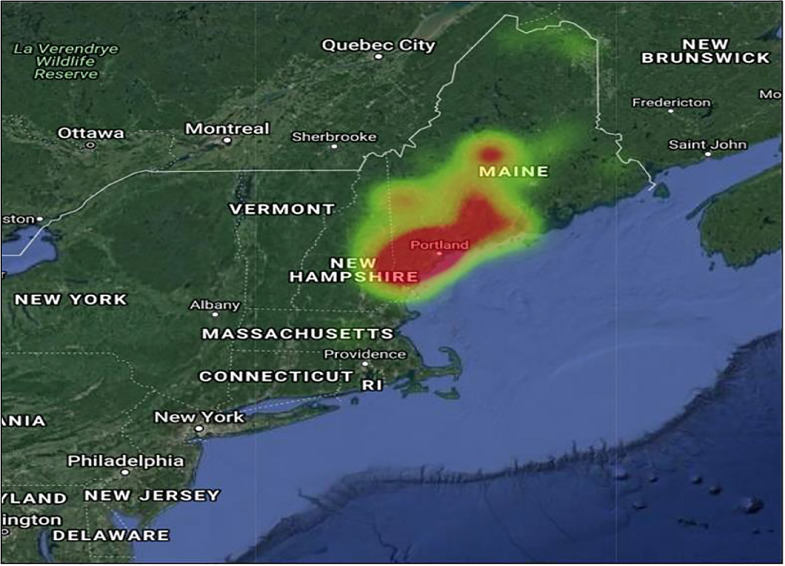
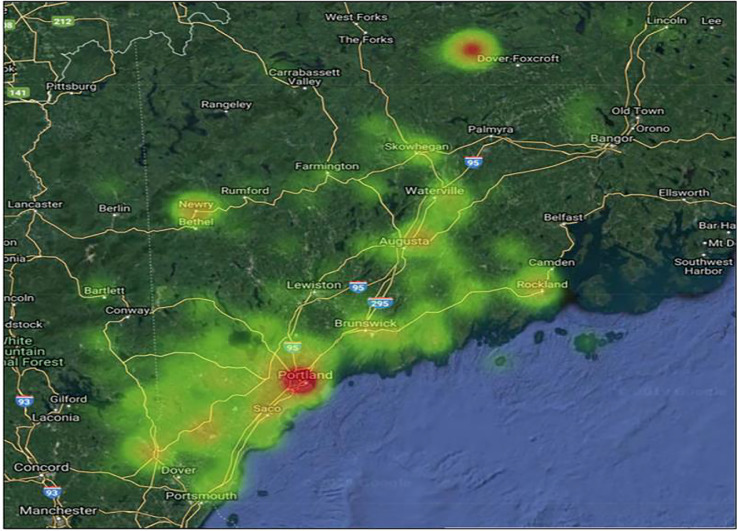
Introduction: In rural settings, factors like weather and location can significantly impact total prehospital time and survival after injury. We sought to determine what prehospital conditions affect mortality and morbidity in severely injured patients.
Materials and methods: We retrospectively evaluated adult trauma patients that were admitted to our level 1 trauma center with Glasgow Coma Score (GCS≤ 9), hypotension (SBP≤ 90 mmHg), or both. Weather and prehospital conditions on patient outcomes were evaluated. Weather data was extracted from the National Oceanographic and Atmospheric Administration public database. Prediction models were done using bivariate and multivariate logistic regression analysis.
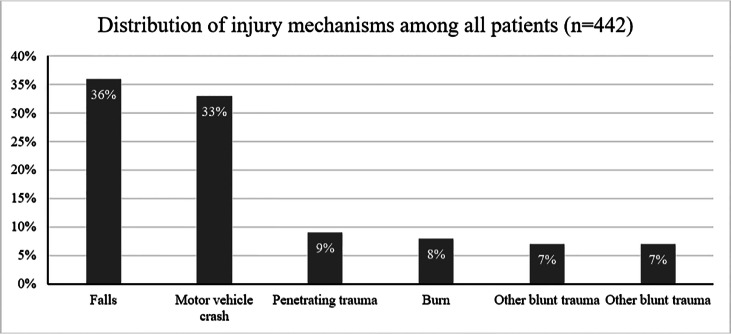
Results: A total of 442 subjects were captured, Median time on the scene was 15 min [IQR =10, 20.5], with median time to definitive care 129 min [IQR= 61, 247]. Hypotension in the field was the greatest predictor of ED mortality (OR=11, P = 0.004), and field hypoxia (OR=3, P = 0.007) was a predictor of in-hospital mortality. Patients with field GCS ≤ 9 had higher odds of ICU admission (OR=2, P = 0.029). Among transfers, increasing prehospital time correlated with ED mortality while injury during warmer weather showed lower odds (OR =0.94, P = 0.019) of mortality. No weather condition predicted mortality for patients that presented directly from the field.
Conclusion: Among severely injured patients being injured during cold weather was associated with higher in-hospital mortality among trauma transfer patients. Prehospital hypotension, hypoxia, and GCS≤9 are also independent predictors of mortality. Future analysis will explore factors impacting transport and field time in order to improve outcomes.
Keywords: Injury; Mortality; Prehospital; Trauma; Weather.
© 2022 The Authors. Published by Elsevier Ltd.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Prehospital factors associated with mortality in injured air medical patients.Prehosp Emerg Care. 2012 Jan-Mar;16(1):121-7. doi: 10.3109/10903127.2011.615011. Epub 2011 Sep 29. Prehosp Emerg Care. 2012. PMID: 21958032
-
A comparison of prehospital and hospital data in trauma patients.J Trauma. 2004 May;56(5):1029-32. doi: 10.1097/01.ta.0000123036.20919.4b. J Trauma. 2004. PMID: 15179242
-
Prehospital intubation for isolated severe blunt traumatic brain injury: worse outcomes and higher mortality.Eur J Trauma Emerg Surg. 2017 Dec;43(6):731-739. doi: 10.1007/s00068-016-0718-x. Epub 2016 Aug 27. Eur J Trauma Emerg Surg. 2017. PMID: 27567923
-
Prehospital Time Following Traumatic Injury Is Independently Associated With the Need for In-Hospital Blood and Early Mortality for Specific Injury Types.Air Med J. 2024 Jan-Feb;43(1):47-54. doi: 10.1016/j.amj.2023.09.013. Epub 2023 Nov 28. Air Med J. 2024. PMID: 38154840
-
Is there an association between female gender and outcome in severe trauma? A multi-center analysis in the Netherlands.Scand J Trauma Resusc Emerg Med. 2019 Feb 13;27(1):16. doi: 10.1186/s13049-019-0589-3. Scand J Trauma Resusc Emerg Med. 2019. PMID: 30760289 Free PMC article.
References
-
- World Health Organization . World Health Organization Press; Geneva: 2010. Injuries and violence: the facts.
LinkOut - more resources
Full Text Sources
