

The Risk Assessment Profile is suboptimal for guiding duplex ultrasound surveillance in trauma patients
- PMID: 39845166
- PMCID: PMC11750042
- DOI: 10.1016/j.sipas.2022.100127
The Risk Assessment Profile is suboptimal for guiding duplex ultrasound surveillance in trauma patients
Abstract
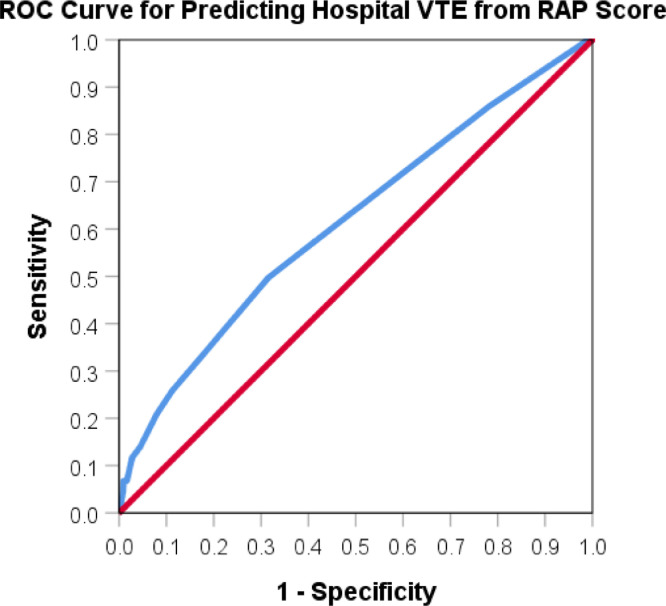
Background: The utility of the Risk Assessment Profile (RAP) score in predicting VTE was assessed, and VTE risk factors identified to guide a duplex ultrasound (DUS) protocol in injured patients.
Methods: Secondary analysis of prospective data on trauma inpatients (March 2017-September 2019), with admission RAP ≥5. Inhospital VTE patients compared to those without. Regression analyses in DVT, PE and proximal DVT, and ROC analysis evaluating RAP's VTE predictability were performed.
Results: 1989 patients were analyzed. VTE was identified in 163(8.2%), DVT 159(8.0%), and PE 10(0.5%) patients. Strongest VTE predictors were massive transfusion (OR 5.97, p = 0.005) and spinal cord injury (OR 2.43, p = 0.03). AUC 0.61 (p < 0.001) on ROC analysis evaluating RAP on VTE. Abdominal injury and major surgery were unique risk factors to non-screened patients.
Conclusion: Performance of RAP to predict VTE was moderate. VTE predictor variables could serve as the foundation for a novel approach guiding DUS surveillance. Derivation and validation are warranted.
© 2022 The Authors. Published by Elsevier Ltd.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Geerts W.H., Code K.I., Jay R.M., Chen E., Szalai J.P. A prospective study of venous thromboembolism after major trauma. N Eng J Med. 1994;331(24):1601–1606. Dec. - PubMed
-
- Adams R.C., Hamrick M., Berenquer C., Senkowski C., Ochsner M.G. Four years of an aggressive prophylaxis and screening protocol for venous thromboembolism in a large trauma population. J Trauma. 2008;65(2):300–308. Aug. - PubMed
-
- Paffrath T., Wafaisade A., Lefering R., Simanski C., Bouillon B., Spanholtz T., Wutzler S., Maegele M. Venous thromboembolism after severe trauma: incidence, risk factors, and outcomes. Injury. 2010;41(1):97–101. Jan. - PubMed
-
- Shackford S.R., Moser K.M. Deep venous thrombosis and pulmonary embolism in trauma patients. J Intensive Care Med. 1988;3(2):87–98.
-
- Rogers F.B., Cipolle M.D., Velmahos G., Rozycki G., Luchette F.A. Practice management guidelines for the prevention of venous thromboembolism in trauma patients: the EAST practice management guidelines work group. J Trauma. 2002;53:142–164. - PubMed
LinkOut - more resources
Full Text Sources
