

Composite dietary antioxidant index is inversely and nonlinearly associated with cardiovascular disease, atherosclerotic cardiovascular disease, and cardiovascular mortality in people with dyslipidemia: evidence from NHANES 2001-2018
- PMID: 39845910
- PMCID: PMC11753228
- DOI: 10.3389/fnut.2024.1478825
Composite dietary antioxidant index is inversely and nonlinearly associated with cardiovascular disease, atherosclerotic cardiovascular disease, and cardiovascular mortality in people with dyslipidemia: evidence from NHANES 2001-2018
Abstract
Background: Dyslipidemia is a major risk factor for cardiovascular disease (CVD) and atherosclerotic CVD (ASCVD). The composite dietary antioxidant index (CDAI), an emerging measure of combined dietary antioxidant exposure, may provide insights into the relationship between diet and CVD/ASCVD outcomes. We aimed to explore the association between CDAI and the prevalence of CVD/ASCVD, as well as CVD mortality in individuals with dyslipidemia.
Methods: CDAI was assessed by integrating dietary vitamins A, C, E, zinc, selenium, and carotenoids. Dyslipidemia was diagnosed according to widely established criteria. Data on CVD/ASCVD were obtained through self-reports, while CVD mortality was obtained through prospective matching participant records with the National Death Index database. Multivariate logistic regression analysis and Cox proportional hazards regression analysis were used to explore these associations and to calculate odds ratios [OR], hazard ratios [HR], and 95% confidence intervals [CI], respectively.
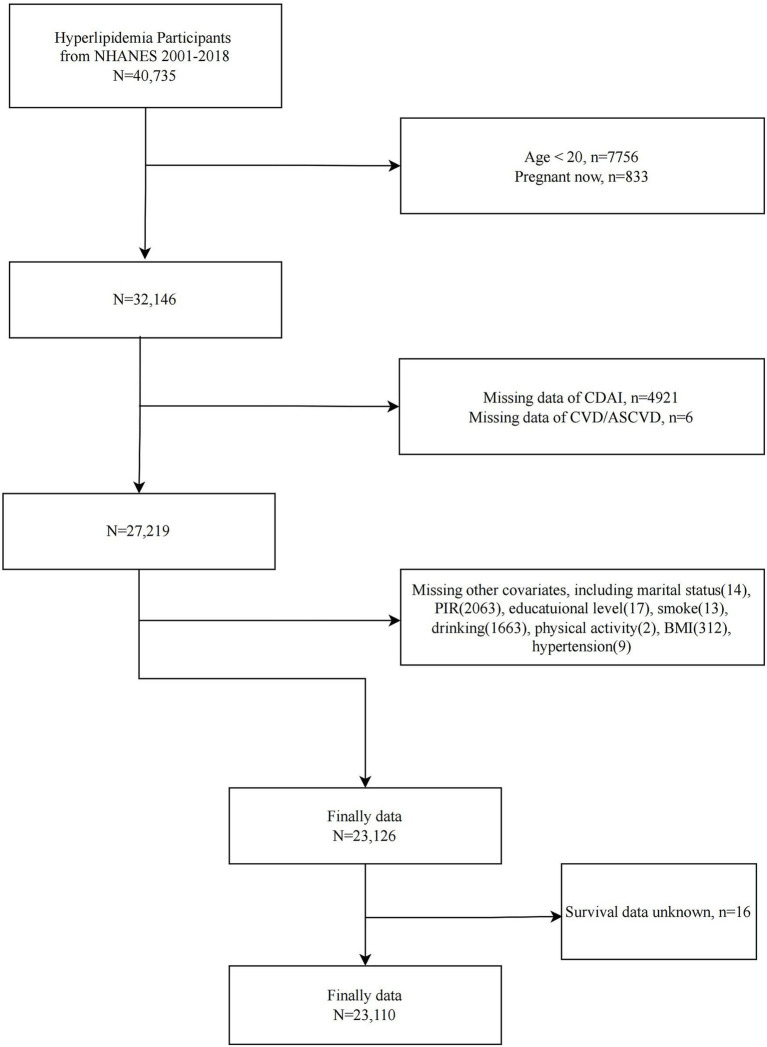
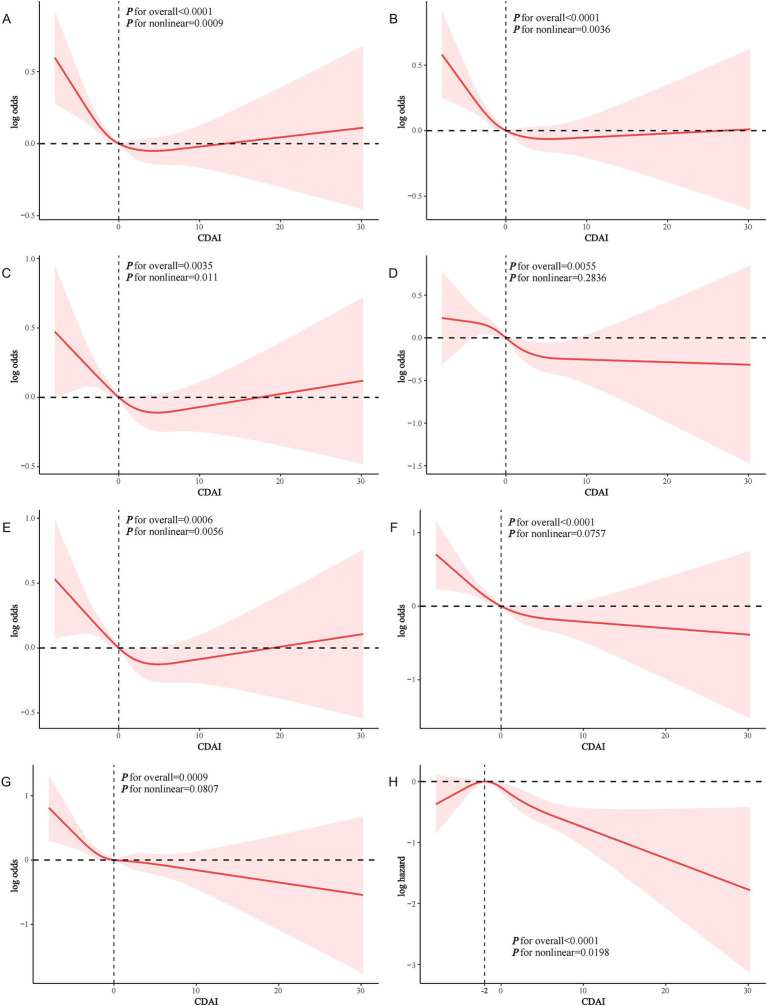
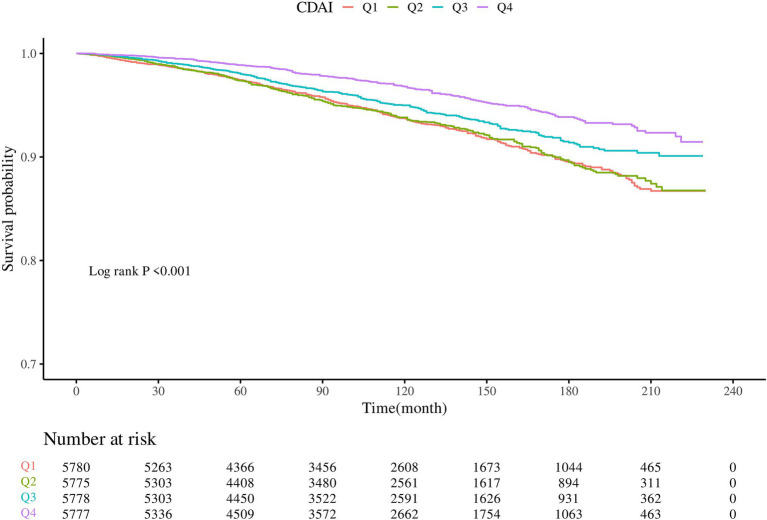
Results: A total of 23,126 participants with dyslipidemia from NHANES 2001-2018 were included. After adjusting for potential confounders, CDAI was inversely associated with the prevalence of both CVD and ASCVD in dyslipidemia populations (OR and 95% CI 0.979 (0.964, 0.995) and 0.977 (0.961, 0.993), respectively). Similar associations were observed between CDAI and specific types of CVD. CDAI was also inversely associated with CVD mortality in dyslipidemia participants (HR = 0.957, 95% CI = 0.939-0.976, p < 0.0001). Restricted cubic spline and threshold effects analyses indicated that CDAI was nonlinearly associated with CVD/ASCVD, with significant associations occurring only when CDAI≤0; however, the association of CDAI with CVD mortality was observed only when CDAI > -2. Furthermore, age, sex, and drinking were found to modify the association of CDAI with CVD/ASCVD, while body mass index influenced the relationship between CDAI and CVD mortality.
Conclusion: CDAI was inversely and nonlinearly associated with both CVD/ASCVD events and CVD mortality in dyslipidemic populations. These findings highlight the potential of antioxidant dietary patterns to alleviate the CVD burden in these populations and underscore the importance of personalized strategies.
Keywords: atherosclerotic cardiovascular disease; cardiovascular disease; cardiovascular mortality; composite dietary antioxidant index; dyslipidemia.
Copyright © 2025 Jiang and Shen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Sarwar N, Danesh J, Eiriksdottir G, Sigurdsson G, Wareham N, Bingham S, et al. . Triglycerides and the risk of coronary heart disease: 10, 158 incident cases among 262, 525 participants in 29 Western prospective studies. Circulation. (2007) 115:450–8. doi: 10.1161/circulationaha.106.637793, PMID: - DOI - PubMed
LinkOut - more resources
Full Text Sources