

Safety or speed? Assessing alternative vascular access for angiography after resuscitative endovascular balloon occlusion of the aorta (REBOA) in severe pelvic trauma patients
- PMID: 39845986
- PMCID: PMC11749535
- DOI: 10.1136/tsaco-2024-001530
Safety or speed? Assessing alternative vascular access for angiography after resuscitative endovascular balloon occlusion of the aorta (REBOA) in severe pelvic trauma patients
Abstract
Introduction: Pelvic fractures often result in life-threatening bleeding and hemodynamic instability. Resuscitative endovascular balloon occlusion of the aorta (REBOA) has emerged as a promising strategy for patients with severe pelvic fractures, facilitating subsequent hemostatic interventions. Transcatheter arterial embolization (TAE) is a well-established procedure for managing pelvic fractures accompanied by hemorrhage.Ideally, an angiographic access point distinct from the initial REBOA placement is sought to maintain REBOA deflation without complete removal, thereby preventing hemodynamic instability during the procedure. However, in cases of extreme and severe pelvic trauma, gaining access for REBOA is already challenging, not to mention the additional difficulty posed by subsequent angiographic access.This study aims to assess the challenges associated with gaining access in cases where successful TAE was ultimately performed, particularly in the context of severe pelvic trauma. We investigate the complexities surrounding access management and its implications for patient outcomes.
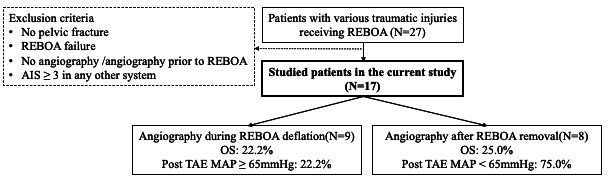
Methods: We conducted a retrospective analysis of patients who presented with pelvic fractures and underwent sequential REBOA and TAE procedures at our institution between 2017 and 2023. We excluded patients with Abbreviated Injury Scores (AIS) ≥3 in systems other than the pelvis, those who underwent TAE prior to REBOA, and cases of suboptimal REBOA insertion.We collected demographic data, injury characteristics, details of the REBOA and TAE procedures, information on complications, and data on patient survival. The primary endpoints of our analysis included overall survival and the success of TAE (defined as post TAE mean arterial pressure (MAP) ≥65 mm Hg). Secondary endpoints encompassed the duration details of two interventions.
Results: Between 2017 and 2023, a total of 17 patients were included in this study. Among this cohort, 12 (70.6%) were male, with a median age of 51 years. Overall survival was 23.5%. Patients were grouped into angiography after REBOA deflation (AAD) or angiography after REBOA removal (AAR). AAR group was younger (39.0 vs 63.0, p=0.030) and had higher Shock Index at triage (2.30 vs 1.10, p=0.015). More patient whose post TAE MAP >=65 mm Hg was found in the AAR group, although no significant difference on overall survival (25.0% vs 22.2%, p=1.000). Angiographic cannulation times, pre-angiographic MAP, and amount of pre-angiographic transfusion of packed red blood cell were similar across groups.
Conclusion: Our findings provide empirical insights into vascular access selection and suggest that AAR in the management of severe pelvic fractures can be beneficial, particularly when pre-angiographic resuscitation is sufficient. Larger studies are required to validate these observations and assess long-term outcomes.
Level of evidence: III.
Keywords: Pelvic Floor; angiography; embolism; resuscitation.
Copyright © Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
none
Figures
References
-
- Cullinane DC, Schiller HJ, Zielinski MD, Bilaniuk JW, Collier BR, Como J, Holevar M, Sabater EA, Sems SA, Vassy WM, et al. Eastern Association for the Surgery of Trauma practice management guidelines for hemorrhage in pelvic fracture--update and systematic review. J Trauma. 2011;71:1850–68. doi: 10.1097/TA.0b013e31823dca9a. - DOI - PubMed
-
- Magnone S, Coccolini F, Manfredi R, Piazzalunga D, Agazzi R, Arici C, Barozzi M, Bellanova G, Belluati A, Berlot G, et al. Management of hemodynamically unstable pelvic trauma: results of the first Italian consensus conference (cooperative guidelines of the Italian Society of Surgery, the Italian Association of Hospital Surgeons, the Multi-specialist Italian Society of Young Surgeons, the Italian Society of Emergency Surgery and Trauma, the Italian Society of Anesthesia, Analgesia, Resuscitation and Intensive Care, the Italian Society of Orthopaedics and Traumatology, the Italian Society of Emergency Medicine, the Italian Society of Medical Radiology -Section of Vascular and Interventional Radiology- and the World Society of Emergency Surgery) World J Emerg Surg. 2014;9:18. doi: 10.1186/1749-7922-9-18. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources