

Performance of computerized self-reported medical history taking and HEAR score for safe early rule-out of cardiac events in acute chest pain patients: the CLEOS-CPDS prospective cohort study
- PMID: 39846077
- PMCID: PMC11750193
- DOI: 10.1093/ehjdh/ztae087
Performance of computerized self-reported medical history taking and HEAR score for safe early rule-out of cardiac events in acute chest pain patients: the CLEOS-CPDS prospective cohort study
Abstract
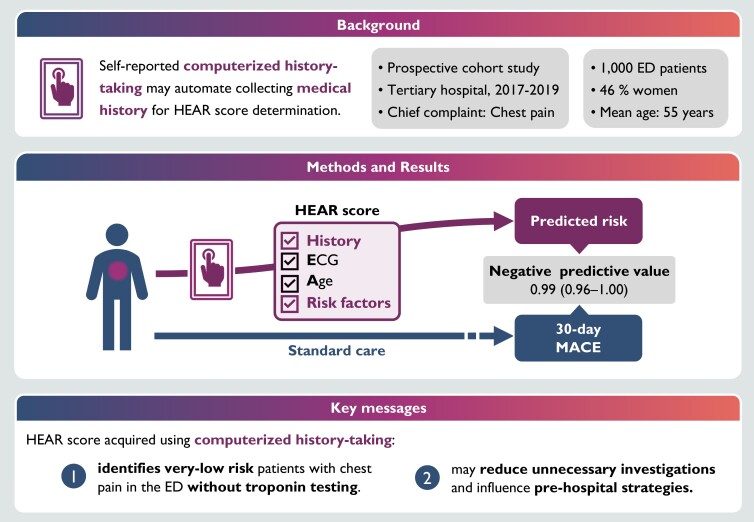
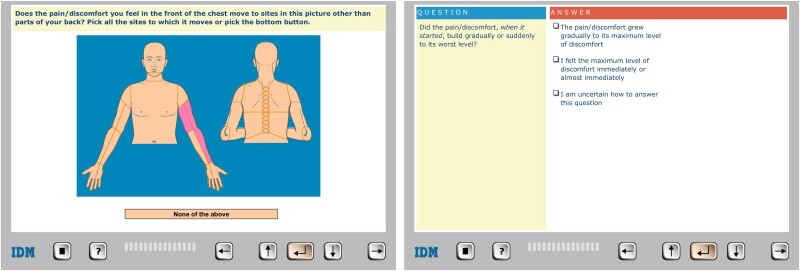
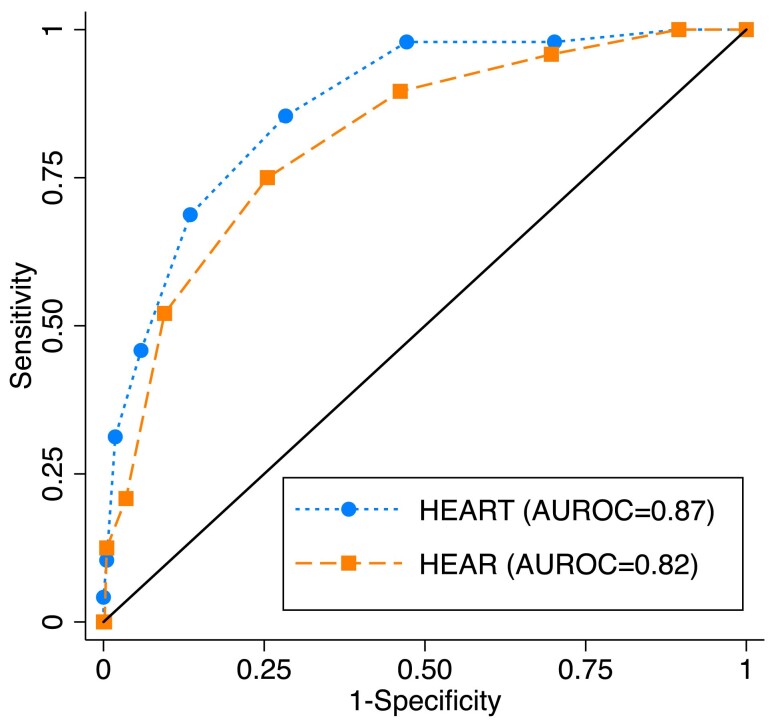
Aims: A simplified version of the history, electrocardiogram, age, risk factors, troponin (HEART) score, excluding troponin, has been proposed to rule-out major adverse cardiac events (MACEs). Computerized history taking (CHT) provides a systematic and automated method to obtain information necessary to calculate the HEAR score. We aimed to evaluate the efficacy and diagnostic accuracy of CHT in calculating the HEAR score for predicting MACE.
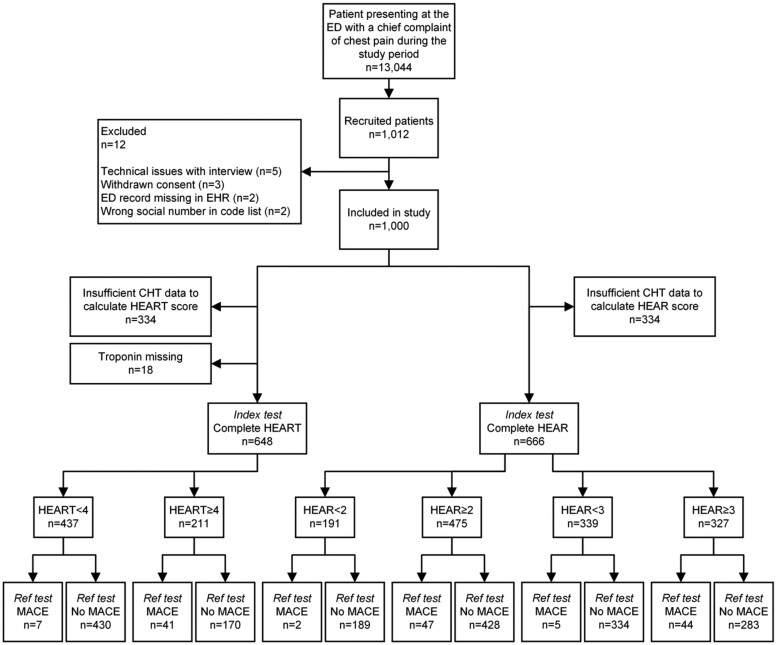
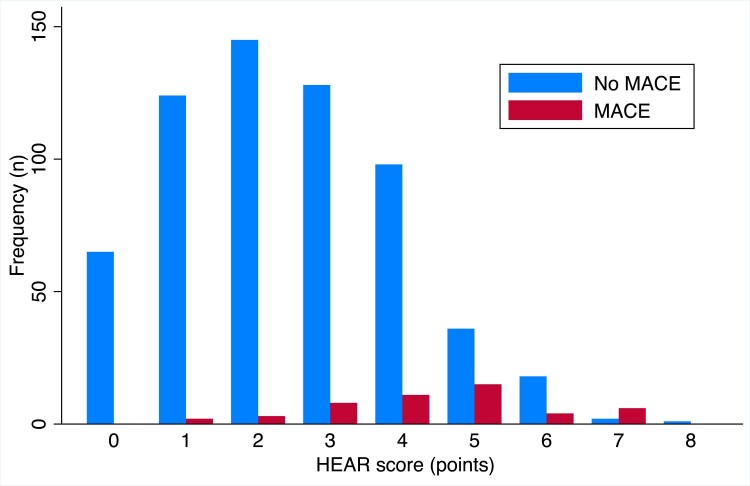
Methods and results: Prospective study including clinically stable adults presenting with chest pain at the emergency department (ED) of Danderyd University Hospital (Stockholm, Sweden), in 2017-19. Participants entered their medical histories on touchscreen tablets using CHT software. The HEAR and HEART scores were calculated from CHT data. Thirty-day MACE and acute coronary syndrome (ACS) outcomes were retrieved, and the diagnostic accuracy was assessed. Logistic regression was used to determine the most predictive components of the HEAR score. Among 1000 patients, HEART and HEAR scores could be calculated from CHT data in 648 and 666 cases, respectively, with negative predictive values [95% confidence interval (CI)] of 0.98 (0.97-0.99) and 0.99 (0.96-1.00). Two patients with HEAR score <2 experienced a 30-day MACE. The age [odds ratio (OR) 2.75, 95% CI 1.62-4.66] and history (OR 2.38, 95% CI 1.52-3.71) components of the HEAR score were most predictive of MACE. Acute coronary syndrome outcomes provided similar results.
Conclusion: The HEAR score acquired by CHT identifies very-low-risk patients with chest pain in the ED, safely ruling out ACS and MACE. This highlights the value of computerized history taking by patients, which may reduce unnecessary tests and hospital admissions.
Trial registration: ClinicalTrials.gov NCT03439449.
Keywords: Artificial intelligence; Chest pain; Coronary artery disease; Medical history taking; Medical informatics; Risk assessment.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: All patent rights and copyrights to technology, language, images, and knowledge content are assigned without royalty rights to Karolinska Institutet, Stockholm, Sweden, which is a public university. T.K.: research grants to Karolinska Institutet from Medtronic, and ReCor Medical; all outside the submitted work. J.S.: speaker honoraria for AstraZeneca, Bayer, NovoNordisk, Medtronic, and shareholder in Beats Vascular Health. All other authors declare no financial or non-financial competing interest.
Figures
References
-
- Fanaroff AC, Rymer JA, Goldstein SA, Simel DL, Newby LK. Does this patient with chest pain have acute coronary syndrome? The rational clinical examination systematic review. JAMA 2015;314:1955–1965. - PubMed
-
- Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A, et al. 2023 ESC guidelines for the management of acute coronary syndromes. Eur Heart J 2023;44:3720–3826. - PubMed
-
- Stepinska J, Lettino M, Ahrens I, Bueno H, Garcia-Castrillo L, Khoury A, et al. Diagnosis and risk stratification of chest pain patients in the emergency department: focus on acute coronary syndromes. A position paper of the Acute Cardiovascular Care Association. Eur Heart J Acute Cardiovasc Care 2020;9:76–89. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical