

Evaluation of Optimized Lumbar Oblique X-Ray Angles with Positioning Assistance for Enhanced Imaging Quality: A Pilot Study in an Asian Cohort
- PMID: 39846664
- PMCID: PMC11755554
- DOI: 10.3390/jfmk10010023
Evaluation of Optimized Lumbar Oblique X-Ray Angles with Positioning Assistance for Enhanced Imaging Quality: A Pilot Study in an Asian Cohort
Abstract
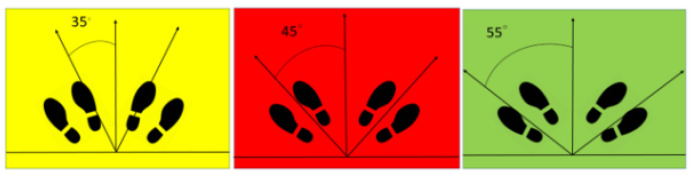
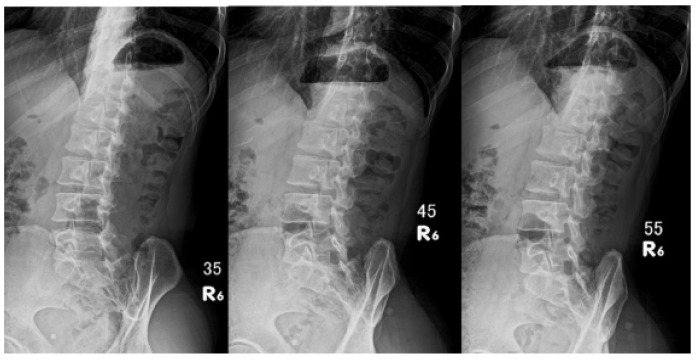
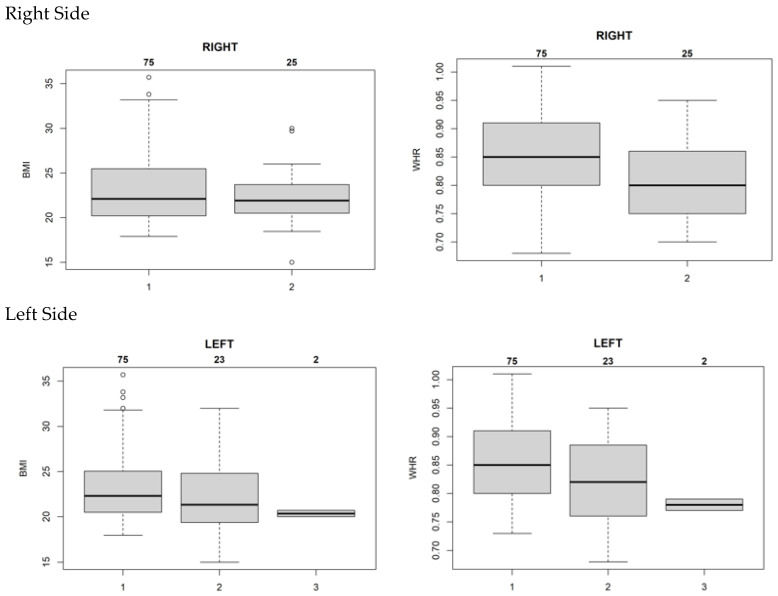
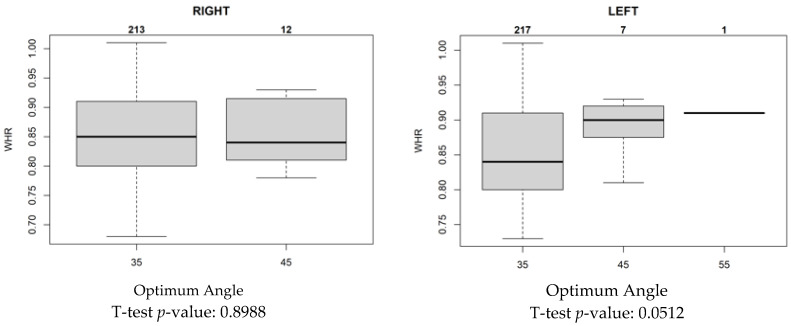
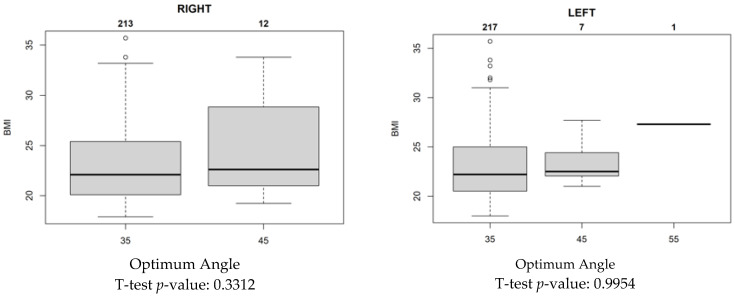
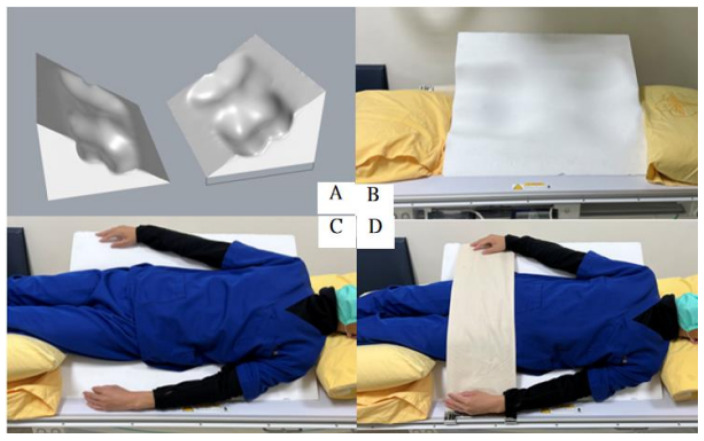
Objective: Pars fractures are a common cause of lower back pain, especially among young individuals. Although computed tomography (CT) and magnetic resonance imaging (MRI) scanning are commonly used in developed regions, traditional radiography remains the main diagnostic method in many developing countries. This study assessed whether the standard radiographic angles suggested in textbooks are optimal for an Asian population since Asian groups have lower lumbar lordosis. This study found a 35° angle to be the most effective angle for lumbar oblique X-ray imaging. Additionally, the potential for a customized positioning auxiliary device was examined to improve image quality and reduce patient discomfort in cost-sensitive healthcare settings like Taiwan's single-payer system. Methods: A total of 100 participants underwent lumbar oblique radiography using a specially designed footboard with angle markings. Radiologists evaluated 600 images based on waist-to-hip ratio (WHR) and body mass index to identify the optimal angulation for various body types. Results: For individuals with a WHR of 0.85, a 35° angle provided superior image quality, while 45° was more effective for slimmer patients. This optimized approach indicates the cost-effectiveness and diagnostic value of traditional X-ray imaging. Conclusions: The 35° angulation standardizes lumbar X-ray imaging for an Asian cohort, reducing repeat scans and improving accuracy. Using a positioning device further enhances image quality and patient comfort, supporting the clinical utility of traditional radiography in resource-limited environments.
Keywords: 3D manufacture; image quality; oblique examination; positioning auxiliary device; spondylolisthesis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Hu S.S., Tribus C.B., Diab M., Ghanayem A.J. Spondylolisthesis and Spondylolysis. J. Bone Joint Surg. Am. 2008;90:656–671. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
