

Improving postsurgical paresis in brain tumor patients by transcranial magnetic stimulation
- PMID: 39847143
- PMCID: PMC11937064
- DOI: 10.1007/s11060-024-04931-9
Improving postsurgical paresis in brain tumor patients by transcranial magnetic stimulation
Abstract
Background and objectives: Recently, reduction of transcallosal inhibition by contralateral navigated repetitive transcranial magnetic stimulation (nrTMS) improved neurorehabilitation of glioma patients with new postoperative paresis. This multicentric study examines the effect of postoperative nrTMS in brain tumor patients to treat surgery-related upper extremity paresis.
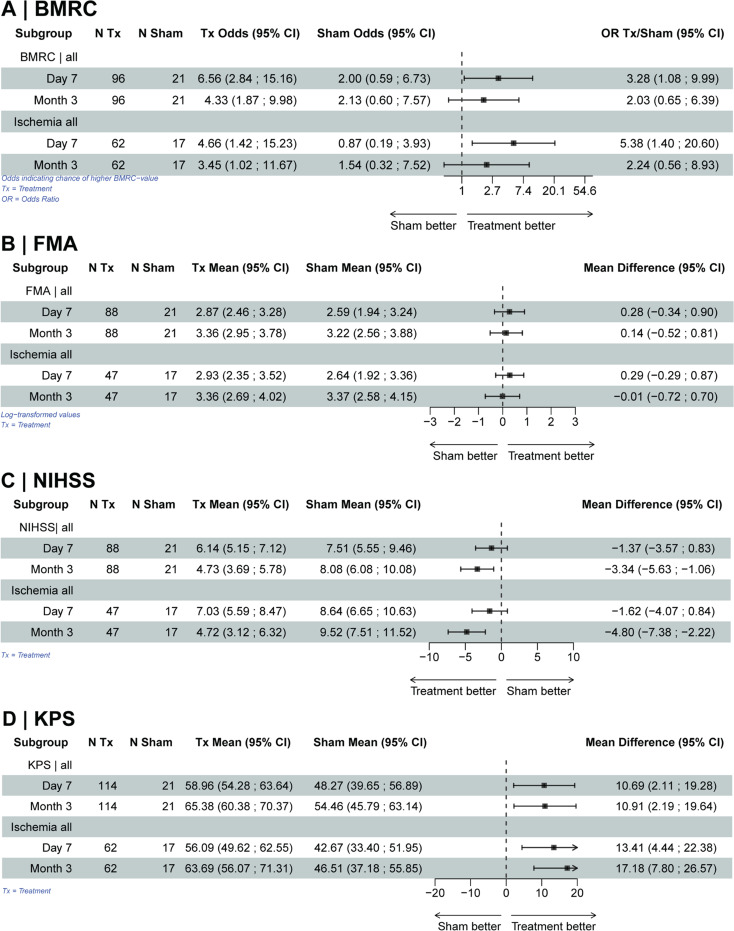
Methods: This is a secondary analysis of two randomized and three one-arm studies in brain tumor patients with new/progressive postoperative paresis. Patients underwent either low frequency contralesional nrTMS or sham stimulation followed by physiotherapy. Outcome was assessed on postoperative day 1, 7, and after 3 months using British Medical Research Council score (BMRC), Fugl-Meyer assessment (FMA), Karnofsky Performance Scale (KPS) and National Institutes of Health Stroke Scale (NIHSS).
Results: A total of 135 patients (mean age of 53.8 years, 60 women) were included, of whom 51 patients were treated in RCTs (30 treatment group, 21 sham group) and 84 in prospective, single-arm studies. Linear mixed models showed an advantage for the treatment group for the BMRC (7 days: OR 3.28; 95%CI: 1.08-9.99; 3 months: OR 2.03, 95%CI: 0.65-6.39) and KPS (7 days: mean difference (MD) 11, 95%CI: 2-19; 3 months: MD 11, 95%CI: 2-20), less pronounced for the FMA (7 days: MD 0.28, 95%CI: -0.34-0.9; 3 months: MD 0.14, 95%CI: -0.52-0.81). A stronger treatment effect was evident with proven ischemia on the postoperative MRI. To observe an improvement by at least one grade at 3 months, the number needed to treat (NNT) for the entire cohort is 4 (BMRC) and 3 patients (KPS), respectively.
Conclusion: Our multicenter data confirm the positive treatment effect of nrTMS to reduce transcallosal inhibition with a considerably low NNT - especially if caused by ischemia.
Keywords: Glioma; Navigated transcranial magnetic stimulation (nTMS); Paresis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organization for the submitted work.BM received honoraria, consulting fees, and research grants from Medtronic (Meerbusch, Germany), Icotec AG (Altstätten, Switzerland), and Relievant Medsystems Inc. (Sunnyvale, CA, USA); honoraria, and research grants from Ulrich Medical (Ulm, Germany); honoraria and consulting fees from Spineart Deutschland GmbH (Frankfurt, Germany) and DePuy Synthes (West Chester, PA, USA); and royalties from Spineart Deutschland GmbH (Frankfurt, Germany). SK is a consultant for Ulrich Medical (Ulm, Germany) and Need Inc. (Santa Monica, CA, USA). TP, SK, SI and BM are consultants for Brainlab AG (Munich, Germany).SI, TP, and SK received honoraria from Nexstim Plc (Helsinki, Finland) for a webinar. TP received research grants from Carl Zeiss Meditec (Oberkochen, Germany) and Olympus Corporation (Center Valley, PA, USA).However, all authors declare that they have no conflict of interest regarding the materials used or the results presented in this study. All authors declare no other relationships or activities that could appear to have influenced the submitted work. Ethical approval: We performed the study in accordance with the Declaration of Helsinki. There were 4 centers involved in this study: Charité – Universitätsmedizin Berlin (I), Technical University of Munich (II), King’s College Hospital, London (III), MD Anderson Cancer Center (IV). The study was conducted as an RCT at 2 sites (I; II), with the study transitioning to a single-arm study at one site after recruitment completion (II). All included patients provided written informed consent at each center. Local ethics boards reviewed and approved the study protocol (registration numbers: Munich NCT03982329 and 12/15, Berlin EA4/132/15, London: 20230701NCR; Houston: NCT03606161). Clinical trial registration/local institutional approval: Munich: NCT03982329, Local institutional registration: 12/15; Berlin: Deutsches Register für klinische Studien (DRKS00010043), Ethics Committee of the Charité (EA4/132/15); London: Local institutional registration 20230701NCR; Houston: NCT03606161.
Figures

References
-
- Gempt J, Forschler A, Buchmann N et al (2013) Postoperative ischemic changes following resection of newly diagnosed and recurrent gliomas and their clinical relevance. J Neurosurg Apr 118(4):801–808. 10.3171/2012.12.JNS12125 - PubMed
-
- McGirt MJ, Mukherjee D, Chaichana KL, Than KD, Weingart JD, Quinones-Hinojosa A (2009) Association of surgically acquired motor and language deficits on overall survival after resection of glioblastoma multiforme. Neurosurg Sep 65(3):463–469 discussion 469– 70. 10.1227/01.NEU.0000349763.42238.E9 - PubMed
-
- Karschnia P, Gerritsen JKW, Teske N et al The oncological role of resection in newly diagnosed diffuse adult-type glioma defined by the WHO 2021 classification: a review by the RANO resect group. Lancet Oncol. 2024;- 25(– 9):- e419. - PubMed
-
- Lefaucheur JP, Aleman A, Baeken C et al (2020) Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): an update (2014–2018). Clin Neurophysiology: Official J Int Federation Clin Neurophysiol Feb 131(2):474–528. 10.1016/j.clinph.2019.11.002 - PubMed
-
- Fridman EA, Hanakawa T, Chung M, Hummel F, Leiguarda RC, Cohen LG (2004) Reorganization of the human ipsilesional premotor cortex after stroke. Brain Apr 127(Pt 4):747–758. 10.1093/brain/awh082 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
