

First-in-human, multicenter, open-label, phase I study of ATOR-1017 (evunzekibart), a 4-1BB antibody, in patients with advanced solid malignancies
- PMID: 39848688
- PMCID: PMC11784162
- DOI: 10.1136/jitc-2024-010113
First-in-human, multicenter, open-label, phase I study of ATOR-1017 (evunzekibart), a 4-1BB antibody, in patients with advanced solid malignancies
Abstract
Background: ATOR-1017 (evunzekibart) is a human agonistic immunoglobulin G4 antibody targeting the costimulatory receptor 4-1BB (CD137). ATOR-1017 activates T cells and natural killer cells in the tumor environment, leading to immune-mediated tumor cell death.
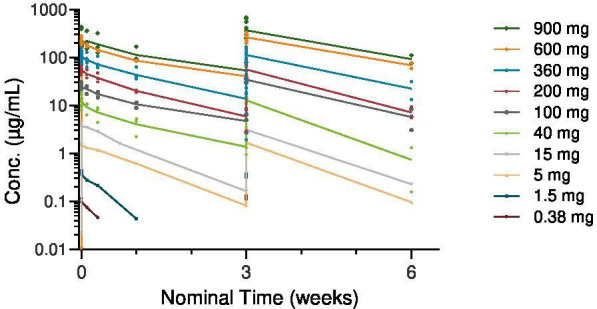
Methods: In this first-in-human, multicenter, phase I study, ATOR-1017 was administered intravenously every 21 days as a monotherapy to patients with advanced, unresectable solid tumors having received multiple standard-of-care treatments. The study used single patient cohorts for rapid dose escalation up to 40 mg; thereafter a modified 3+3 design up to 900 mg. Escalating doses were given until disease progression, unacceptable toxicity, or withdrawal of consent. The primary objective of the study included determination of the maximum tolerated dose (MTD) via assessment of adverse events and dose-limiting toxicities (DLTs). Secondary objectives included determination of the pharmacokinetics, immunogenicity and clinical efficacy assessed with CT scans using immune Response Evaluation Criteria in Solid Tumors. Exploratory objectives included pharmacodynamic (PD) assessment of immune system biomarkers.
Results: Of the 27 patients screened, 25 received treatment with ATOR-1017. The median time on study was 13.1 weeks (range 4.3-92.3). The MTD of ATOR-1017 was not reached. Treatment-related adverse events (TRAEs) were reported in 13 (52%) of 25 patients; most common (≥10%) were fatigue (n=4 (16.0%) patients) and neutropenia (n=3 (12.0%) patients). Five patients experienced a severe (≥ grade 3) TRAE; neutropenia (n=2), febrile neutropenia (n=1), chest pain (n=1), increased liver enzymes (n=1), and leukopenia and thrombocytopenia (n=1). No patients discontinued due to TRAEs and no DLTs were observed. Pharmacokinetic data demonstrated approximate dose-proportional kinetics. Dose-dependent increases in PD biomarkers, including soluble 4-1BB, are indicative of target-mediated biological activity. Best response was stable disease in 13 out of 25 patients (52%), maintained for 6 months or longer in six patients (24%).
Conclusions: Treatment with ATOR-1017 was safe and well tolerated at all dose levels and demonstrated biological activity. Furthermore, almost one-third of patients experienced long-lasting stable disease in this heavily pretreated population. The encouraging safety and preliminary efficacy data warrant further clinical development of ATOR-1017, possibly in combination with other anticancer agents.
Keywords: Antibody; Solid tumor.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: GU reports consulting fees from Alligator Bioscience AB and is a member of the board for the Swedish Guidelines for Cutaneous Malignant Melanoma and the Swedish Cancer fun. AC and AH report no conflict of interest. KES, PE, and SVA are employees of Alligator Bioscience, AB. LS was an employee of Alligator Bioscience, AB at the time of the study.
Figures



References
-
- Melero I, Sanmamed MF, Glez-Vaz J, et al. CD137 (4-1BB)-Based Cancer Immunotherapy on Its 25th Anniversary. Cancer Discov. 2023;13:552–69. doi: 10.1158/2159-8290.CD-22-1029. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials